
-
Mail us:
editor@raftpubs.org
Indexing & Abstracting
Full Text
Case ReportDOI Number : 10.36811/osjs.2019.110009Article Views : 29Article Downloads : 32
Peritonitis by Spontaneous rupture of ovarian dermoid cyst: a case report
Diallo AC1,3*, Tendeng JN1, Ndong A1, Diao ML1, Thiam O2, Thiam JA3, Dia DA1, Diouf A2, Sow DB2, Sarr CT2, Manyacka PM1, Ka S3 and Konate I1
1Department of Surgery, Gaston Berger University, Saint-Louis, Senegal
2Department of Gynecology and Obstetrics, Saint-Louis Hospital, Senegal
3Joliot Curie Institute, Dakar, Senegal
*Corresponding Author: Adja Coumba Diallo, Department of Surgery, Gaston Berger University, Saint-Louis, Senegal, Email: coumbisadja@yahoo.fr
Article Information
Aritcle Type: Case Report
Citation: Diallo AC, Tendeng JN, Ndong A, et al. 2019. Peritonitis by Spontaneous rupture of ovarian dermoid cyst: a case report. Open Sci J Surg. 1: 60-62.
Copyright: This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Copyright © 2019; Diallo AC
Publication history:
Received date: 09 December, 2019Accepted date: 13 December, 2019
Published date: 16 December, 2019
Abstract
Background: Ovarian dermoid cyst is a benign congenital tumor. It is often incidentally diagnosed and can be revealed in very rare cases by spontaneous rupture. We report the case of a ruptured ovarian dermal cyst complicated by generalized peritonitis.
Case report: This was a 20-year-old female patient, who consulted for abdominal pain associated with fever and vomiting. Physical examination found generalized abdominal contracture. Plain abdominal radiography found pneumoperitoneum. Biology showed leukocytosis at 18000 / mm3. Median laparotomy revealed a collection 2000 cc of pus with a ruptured right ovarian mass. An adnexectomy with lavage of abdominal cavity were performed. Anatomopathological examination concluded to an ovarian dermoid cyst with no sign of malignancy. The postoperative course was uneventful.
Conclusion: Rupture of a dermoid cyst of the ovary is a rare acute complication. Examination of the operative specimen is mandatory to eliminate malignancy.
Keywords: Ovary; Dermoid cyst; Rupture; Acute complication; Peritonitis; Ovary
Introduction
The dermoid cyst or mature cystic teratoma of the ovary is a benign, congenital tumor [1]. It evolves at the expense of pluripotent germ cells capable of constituting tissues derived from the 3 embryonic leaves (ectoderm, endoderm, mesoderm) [2]. It is often incidentally diagnosed but can be revealed in very rare cases by a spontaneous rupture. We report the case of a rupture ovarian dermoid cyst complicated by generalized peritonitis.
Case report
It was a 20-year-old patient who consulted for abdominal pain that had been evolving for 2 weeks. These symptoms were associated with fever and vomiting. Physical examination found a generalized abdominal contracture. Plain abdominal radiography showed pneumoperitoneum (Figure 1). At the blood count, leukocytosis at 18000 / mm3 was noted. A median laparotomy was performed. On exploration, there was a collection estimated to 2000 cc of purulent fluid with a ruptured right ovarian mass. An adnexectomy with peritoneal lavage were done. The macroscopic appearance of the operative specimen was in favor of an ovarian teratoma with the presence of hair and teeth (Figure 2). The postoperative course was uneventful with discharge on the 5th day. Histopathology concluded to a mature teratoma of the ovary without signs of malignancy.
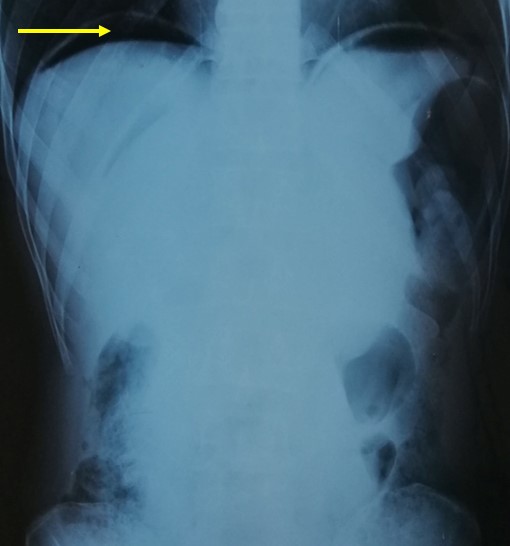
Figure 1: Plain abdominal radiography with pneumoperitoneum (arrow).
Discussion
The dermoid cyst of the ovary represents 11-25% of ovarian tumors [3]. It is rarely complicated (4 to 6% of cases). The most common complication is torsion (15%) [4]. The rupture in peritoneal cavity is a very rare complication estimated at 1.3% [5]. Spontaneous rupture is rarer because most reported case are iatrogenic during laparoscopy [3]. Ultrasonography can help in the diagnosis. Dermoid cysts often appear as a cystic formation with an echogenic nodule attached to its wall (the Rokitansky nodule) [6]. However, CT or MRI, the presence of fat is the main element that allows diagnosis in most cases [1]. A malignant transformation is possible but rare. It is observed especially after menopause [7]. Complete rupture of dermoid cyst lead to chemical peritonitis [8]. Symptoms depends on the type of the rupture: localized or generalized peritonitis [9,10]. Contact between contents of the cyst and peritoneum is responsible for an inflammatory reaction [4]. And in this case, it causes granulomatous peritonitis which have poor prognosis [5]. Treatment usually consists of a resection of the cyst or adnexectomy [11]. This was the case with our patient. Peritonitis after spontaneous or iatrogenic rupture may have poor prognosis [12]. Indeed, it can cause sepsis by infection or adhesions at the origin of intestinal obstruction. An early diagnosis and treatment help to improve the prognosis.

Figure 2: Ovarian teratoma with the presence of hair (red arrow) and teeth (yellow arrow).
Conclusion
Spontaneous rupture of dermoid ovarian cyst is a rare complication that can lead to generalized peritonitis. Surgical management requires cystectomy or adnexectomy with peritoneal lavage. Prognosis is generally favorable with early diagnosis and treatment.
References
1. Damarey B, Farine MO, Vinatier D, et al. 2010.Tératomes ovariens matures et immatures : caractéristiques en échographie, TDM et IRM. J Radiol. 91: 27?36. Ref.: https://rb.gy/isefr2
2. Alleman I, Couvert-Mullot H, Béranger C, et al. 2010. Prise en charge du cancer du sein en cas de récepteurs hormonaux négatifs. Pharm Hosp. 45: 25?32. Ref.: https://rb.gy/yhsuqf
3. Nezhat C, Kalyoncu S, Johnson E, et al. 1999. Laparoscopic management of ovarian dermoid cysts: Ten years’ experience. Obstet Gynecol. 3: 179-184. Ref.: https://rb.gy/jmvlom
4. ABDELKEFI MS. 2014. Kyste dermoïde de l’ovaire compliqué d’une péritonite chimique : A propos d’un cas. La Tunisie chirurgicale. 24.
5. Rubod C, Triboulet JP, Vinatier D. 2007. Kyste dermoïde de l’ovaire compliqué d’une péritonite chimique. À propos d’un cas. Gynécologie Obstétrique Fertil. 35: 651?653. Ref. : https://bit.ly/2PftlHJ
6. Hertzberg BS, Kliewer MA. 1996. Sonography of benign cystic teratoma of the ovary: pitfalls in diagnosis. Am J Roentgenol. 167: 1127?33. Ref. : https://bit.ly/3496S3a
7. Argoitia X, Duga I, Labeyrie E, et al. 2007. Dégénérescence des kystes dermoïdes. À propos d’un cas de transformation maligne. Gynécologie Obstétrique Fertil. 35: 1005?1008. Ref. : https://bit.ly/2slRtPG
8. Yaka M, Ehirchiou A, Alkandry S, et al. 2015. Kyste dermoïde géant de la paroi abdominale: une observation rare. 21. Ref.: https://bit.ly/2t8F2ap
9. Narducci F, Orazi G, Cosson M. 2001. Kyste ovarien: indications chirurgicales et voies d’abord. Ref.: https://bit.ly/38q9ixP
10. Simillis C, Cribb E, Gurtovaya Y, et al. 2019. Generalised purulent peritonitis and small bowel obstruction due to a spontaneously perforated ovarian dermoid cyst. BMJ Case Rep. 12. Ref.: https://bit.ly/35gLlXD
11. Rantomalala HYH, Raveloson JR, Rakotoarisoa B, et al. 2003. Une fistulisation vésicale d’un kyste dermoïde de l’ovaire. Ann Urol. 37: 102?104. Ref. : https://bit.ly/2LNPryH
12. Shamshirsaz AA, Shamshirsaz AA, Vibhakar JL, et al. 2011. Laparoscopic management of chemical peritonitis caused by dermoid cyst spillage. JSLS. 15: 403?405. Ref. : https://bit.ly/2PGyqb7


















