
-
Mail us:
editor@raftpubs.org
- ISSN : 2583-1534
Indexing & Abstracting
Full Text
Research ArticleDOI Number : 10.36811/ojrmi.2020.110006Article Views : 24Article Downloads : 23
Assessment of the Awareness and Attitude of Emergency Physicians towards the use of Computed Tomography in patients with head injury in various hospitals in Anambra State, Nigeria
Okechukwu Mary-Ann C
Imaging Scientist, Federal Medical Center Gusau, Nigeria
*Corresponding Author: Okechukwu Mary-Ann C, Federal Medical Center, P.M.B 1008 Sokoto Bye-Pass road, Gusau, Zamfara State Nigeria, Tel: +2348108545344; Email: okechukwuchidinma@yahoo.co.uk
Article Information
Aritcle Type: Research Article
Citation: Okechukwu Mary-Ann C. 2020. Assessment of the Awareness and Attitude of Emergency Physicians towards the use of Computed Tomography in patients with head injury in various hospitals in Anambra State, Nigeria. O J Radio Med Img. 3: 01-14.
Copyright: This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Copyright © 2020; Okechukwu Mary-Ann C
Publication history:
Received date: 26 November, 2019Accepted date: 23 January, 2020
Published date: 24 January, 2020
Abstract
The use of x-ray and computed tomography scan is critical in the management of traumatic conditions, particularly head injuries. This study was carried out to assess the level of awareness and attitude of Emergency physicians towards the use of CT in cases of head injury. A cross-sectional study was done among emergency physicians working in five different government hospitals in Anambra State. Among the respondents were 29% males and 4% females: mean age was 35.7 years while their modal age was 31-40 years. All the respondents, 33 (100%) stated they find CT scan as a useful diagnostic medical imaging modality. However less than half of them, 15 (45.5%) stated they refer patients for CT scan for those patients that need it. Whereas most of them, 20 (64.5%) stated that head injury patients should undergo both X-Ray and CT scan virtually all of them 32 (97%), responded that computed tomography, (CT) is better than skull x-ray in the examination of head injury. Though majority of the respondents 31 (93%), stated that CT scan subject the patient to some risks. All those who responded and thought that CT scan should continue to be used as medical diagnostic imaging modality were 33 (100%). The result of the study showed that most of the emergency physicians are aware of the usefulness of CT in the examination of patients presenting with head injury, but the non- availability and cost of services of the CT imaging equipment greatly affected the rate of request for the examination and has affected their attitude towards the use of this imaging modality in the examination of this category of patients in need of it.
Introduction
Computed tomography (CT) is a diagnostic imaging procedure used to create detailed images of internal organs, bones, soft tissue and blood vessels. Also referred to as computed axial tomography or computerized axial tomography or computerized tomography CT tomography is a type tomography in which a three-dimensional image of a body structure is constructed by computer from a series of plane cross-sectional images made along an axis. This technique offers better diagnostic results and evaluation of the emergency nature of the patient's condition and enhances resolution in demonstrating intracranial hemorrhage and cerebral infarction in head injuries [17]. An emergency physician is a physician who works at an emergency department to care for acutely ill patients. The emergency physician is a specialist in advanced cardiac life support (advanced life support in Europe), resuscitation, trauma care such as fractures and soft tissue injuries, and management of other life-threatening situations [24]. Head Injury refers to traumatic head injuries, such as those suffered during falls, accidents and other blows to the head. It may or may not include injury to the brain, and it can be as a result of closed or open injuries in the head [1]. Head injury or head trauma encompasses a wide variety of injuries with differing severities, ranging from trivial head wounds to traumatic brain injuries. In the United States, a large emphasis has been placed on traumatic brain injuries (TBIs). Head injuries or what other researchers called traumatic brain injury, (TBI) is one of the leading causes of death and disability among children and adults in their most productive years. Research has shown that nearly 1.6 million head injuries occur annually in the United States, with over 250,000 of these patients being admitted to hospitals [16]. More recent studies showed that in the USA approximately 1.7 million people sustain a TBI annually, about 1.365 million, (80%) are treated and released from an emergency departments of USA hospitals; 275,000 of them are hospitalized while 52,000 die from TBI-related causes. This makes TBIs to be very important public health challenges as they contribute to a third (30.5%) of all injury related deaths in the United States alone [7]. Motor vehicle accidents are the most common cause of closed head injuries and are especially common in teenagers and young adults while falls are responsible for the most injuries among the extremes of young and old age groups. The most common causal factors for head injury include road traffic accidents (RTA), physical assaults, falls from heights and stab wounds. Concussion and unconsciousness are often immediate results of traumatic head injury. The long-term effects of head injury can be manifested in a variety of learning, speech, memory, and behavior problems (Encarta, 2008). The radiological examinations requested for a patient with head injury is usually a skull x-ray examination and/or computed tomography examination of the head. Diagnostic imaging of head injuries had traditionally relied on the use of skull radiography [16]. Prior to the emergence and widespread use of Computerized Tomography, CT and magnetic resonance imaging, MRI, plain skull radiography has been used extensively to localize wound sites or penetrating objects, and predict intracranial injury. These neuroimaging techniques provide some of the most important diagnostic, pathophysiologic and prognostic information in the management of patients with head injury, they find diagnostic value in many types of head injury including penetrating brain injuries (PBI), [15]. While bullets are the most common foreign bodies in PBI, chopsticks, toothbrushes, nails and knives have also been reported. Foreign bodies into the cranium pose immediate complications, such as pneumocephalus, intracerebral hemorrhage, contusions and brain stem injury, which, in the short to medium term sequelae, can lead to abscesses, meningitis and encephalitis. Historically, x-ray examination of the skull has been used as a standard radiological procedure in the evaluation of patients with head injury. Skull radiography is useful for imaging of fractures, penetrating injuries, and radiopaque foreign bodies. The skull x-ray has been criticized as an overused and not very valuable radiological procedure due to the drawbacks it was seen to have. However, there are low yield of abnormal findings in these skull x-rays diagnostic techniques [2].
Other drawbacks of x-rays as diagnostic imaging techniques have been summarized by, (Carroll, 2004) to include the following:
• Low yield of positive skull x-rays and low sensitivity of the skull x-ray in detecting clinically important intracranial abnormalities such as subdural hematoma and cortical atrophy.
• Failure in detecting a fracture in the absence of any clinical evidence of intracranial damage,
• The use of a non-invasive diagnostic imaging technology that offers vastly superior information on intracranial disease and injury namely, the computed tomography scanner.
These draw-backs led to the search for better diagnostic imaging techniques for use in the management of patients with head injuries. Such modern techniques as computed tomography, (CT) and magnetic resonance imaging, (MRI) have emerged as better alternatives to x-rays. Computed tomography plays a very important role in the management of the patients with head injury [1]. It provides non- invasive and accurate means of demonstrating both the immediate and delayed features of head injury. However, there is much controversy about the use of computed tomography (CT) for patients with minor head injury [19]. Many institutions have set up Clinical Decision Rules that guide emergency physicians on whether or not to request for CT scans for a patient. These rules tend to checkmate a possible misuse of the scan. (Rohacek et al, 2005) hypothesized that institutional guidelines are not frequently used, and that psychological factors are a common reason for ordering an unnecessary CT. Advantages of CT (when available) for evaluation of the head-injured patient include its high sensitivity in demonstrating mass effect, ventricular size and configuration, bone injuries, and acute hemorrhage regardless of location (i.e., parenchymal, subarachnoid, subdural, or epidural spaces), rapidity of scanning, and compatibility with other medical and life support devices. Radiographers frequently apply tomographic imaging to aid diagnosis and assess the treatment outcomes of traumatic conditions particularly head injuries. Hence this project seeks to study the awareness and attitude of emergency physicians towards the use of computed tomography (CT) in patients with head injury in various teaching hospitals in Anambra state, Nigeria in order to generate evidence-based research information that would facilitate the development of improved application of CT techniques in patient care. This type of study is necessary in order to generate data that would aid in assessing the level of the utilization of CT as important diagnostic equipment for patients with head injury, as well as creating awareness for the importance of CT in places where it is being neglected. This study will define the reasons for the non-regular use of CT as an investigative tool on patients with head injury as well as and other associated factors for the use of this procedure. This would help to identify practice gaps that could be improved to ensure better services delivery and patients' safety. This study was limited to the emergency units in hospitals in Anambra state. It involved physicians working in various hospitals in Anambra State Nigeria. A total of five hospitals in the state were included in the study.
Computed Tomography
Computerized tomography (CT) scan uses X-rays and a computer to create detailed images of the inside of the body. They are carried out in hospital by specially trained operators called radiographers and can be done while you're staying in hospital or during a short visit. CT scans produce detailed images of many structures inside the body, including the internal organs, blood vessels and bones and they are used to:
• Make diagnosis in health conditions particularly those that involve damage to bones, injuries to internal organs, problems with blood flow, strokes and cancer
• Guide further tests or treatments; for example, CT scans can help to determine the location, size and shape of a tumor before having radiotherapy, or allow a doctor to take a needle biopsy (where a small tissue sample is removed using a needle) or drain an abscess.
• Monitor treatment progress of health conditions such as checking the size of tumors during and after cancer treatment
Fundamentally the CT scan are useful for acquiring and reconstructing an image of a thin cross section of an object [11,3]. It is a diagnostic procedure that uses special x-ray equipment to obtain cross-sectional pictures of the body [5]. The CT computer displays these pictures as detailed images of organs, bones, and other tissues. This procedure is also called CT scanning, computerized tomography, or computerized axial tomography (CAT). It differs from conventional projection in two significant ways: First, CT forms a cross-sectional image, eliminating the superimposition of structures that occurs in plane film imaging because of compression of 3D body structures onto the two-dimensional recording system. Second, the sensitivity of CT to subtle differences in x-ray attenuation is at least a factor of 10 higher than normally achieved by screen- film recording systems because of the virtual elimination of scatter [10].
Multi-detector computed tomography scanning is now widely available and recommended as the diagnostic imaging modality of choice for penetrating brain injury, allowing both vascular assessment and evaluation of the craniofacial skeleton and viscera of the head [6]. CT is advantageous over other imaging modalities due to it being readily available, able to acquire images quickly, sensitivity for head injuries and high image resolution available with thin-section acquisitions [23,15]. One of the major advantages of the CT imaging is the ability to visualized three-dimensional images of scanned structures such as the following CT 3-D images shown below [23].
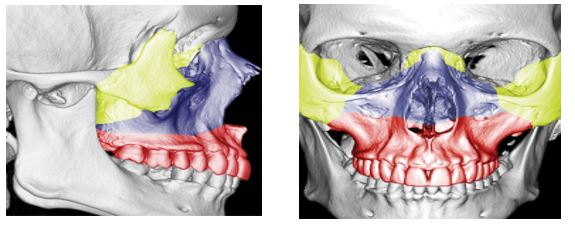
Three dimensional CT images of an adult skull in frontal (a) and lateral (b) orientations with colour overlays show the osseous facial structures that are typically affected by type I (red), type II (blue), and type III (yellow) of Le Fort fractures.
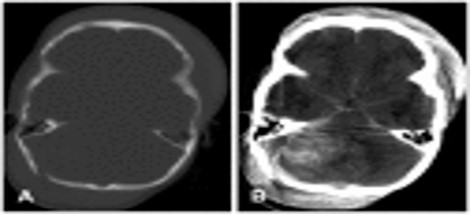
Computed tomography scan of the head showing a depressed fracture penetrating the superior sagittal sinus (A) and hemorrhagic contusion of the parenchyma (B).
Procedure undertaken during CT
During a CT scan, the person lies very still on a table. The table slowly passes through the center of a large x-ray machine. The person might hear whirring sounds during the procedure. People may be asked to hold their breath at times, to prevent blurring of the pictures.
Patient undergoing CT of the abdomen. Drawing shows the patient on a table that slides through the CT machine, which takes x-ray images of the inside of the body.
Often, a contrast agent, or "dye," may be given by mouth, injected into a vein, given by enema or given in all three ways before the CT scan is done. The contrast dye can highlight specific areas inside the body, resulting in a clearer picture.
Computed tomography scans do not cause any pain. However, lying in one position during the procedure may be slightly uncomfortable. The length of the procedure depends on the size of the area being x-rayed; CT scans take from 15 minutes to 1 hour to complete. For most people, the CT scan is performed on an outpatient basis at a hospital or a doctor's office, without an overnight hospital stay.
Risks associated with CT scan
There are general concerns about the risks associated with CT scans particularly in relation to the amount of radiation patients are exposed to during a CT scan. Though radiation exposure from a CT scan could be higher than from a regular x-ray the risks of not having the procedure may be more than having it, especially if cancer is suspected. Physicians considering CT scan must weigh the risks and benefits of the procedure. Generally, CT scan is a very low-risk procedure. The most common problem is an adverse reaction to intravenous contrast-media materials particularly the dyes. Iodine-based contrast media are frequently used to make many organs and structures, such as the kidneys and blood vessels, much more visible on the CT scan tomography. There may be itching, a rash, hives, or a feeling of warmth throughout the body due to the contrast media used, but they are usually self-limiting reactions that resolve rather quickly. Antihistamines may be given to relieve the symptoms where necessary.
A more serious allergic reaction to intravenous contrast is called an anaphylactic reaction. When this occurs, the patient may experience severe hives and/or extreme difficulty in breathing. Affected patients may experience mild itching or hives (small bumps on the skin) symptoms of a more serious allergic reaction include shortness of breath and swelling of the throat or other parts of the body. Such patients should be counseled to tell the technologist or physician immediately if they experience any of these symptoms for prompt treatment. Such reaction is quite rare, but is potentially life-threatening if not treated. Medications which may include corticosteroids, antihistamines, and epinephrine can reverse this adverse reaction. Nephrotoxicity which can result in kidney failure is an extremely rare complication of the intravenous contrast material used in CT scans. People with diabetes, people who are dehydrated, or patients who already have impaired kidney function are most prone to this reaction. Newer intravenous contrast agents have been developed, such as Isovue, which have nearly eliminated this complication. Most physicians suggest that all radiation exposure to patients should be kept to a minimum; those patients that "doctor shop" or repeatedly go to emergency departments for a "CT" put themselves at risk for radiation-caused problems.
Materials and Methods
A prospective, cross-sectional survey research was adopted for this study. The target population for this study comprises practicing emergency physicians in the various government hospitals in Anambra State namely; Nnamdi Azikiwe University Teaching Hospital (NAUTH), Chukwuemeka Odumegwu Ojukwu Teaching Hospital Amaku, Iyienu Mission Hospital Ogidi, St. Charles Borromeo Hospital Onitsha, General Hospital Onitsha. The estimated total population of emergency physicians practicing in the various government hospitals in Anambra State was gotten from the hospitals' record for the emergency physicians and is given as follows; NAUTH Nnewi has (11), NAUTH Neni has (5), Amaku has (7), Iyienu has (10), St. Charles has (5), General Hospital has (4) giving a total of (42) emergency physicians in the various selected government hospitals in Anambra State. Of the 42 emergency physicians, 9 of them were either on annual leave or on outside posting leaving us with 33 emergency physicians present during period of the study. Structured questionnaires were used for data collection. It was designed in line with the objectives of study. The questions were well written in English language and had both closed and open-ended questions. The questionnaire contained a total of 28 questions, divided into three sections: sections A, B, and C. Section A contained questions on the physicians' personal data, section B contained 16 questions aimed at determining the level of knowledge of the physician towards the use of CT in patients with head injury. Section C contained 10 questions aimed at determining the factors affecting the attitude of the emergency physicians towards the use of CT in patients with head injury.
Data Analysis
Data was analyzed using the Statistical Package for Social Sciences (SPSS) version 20. Of the 38 questionnaire instruments administered to the respondents, 33 were completed and returned to the researcher; response rate: 87%. Among the respondents were 29% males and 4% females. There means age as at last birthday was 35.7 years (SD: 7.2 years) while their modal age was 31-40 years. Their Mean age of practice in their respective hospitals was 6.6 (SD: ± 4.4) years while the modal range of years of practice: 1-5 Years. More than half of the respondents, 18 (54.5%) of the respondents were employed in teaching hospital while the rest, 15 (45.5%) were working in state government General hospital or Mission hospital within the state. The rest of the demographic characteristics are presented in the table below.
|
Table 1: Demographic Characteristics of Respondents. |
|||
|
Variables |
Proportion of Respondents |
||
|
Male |
Female |
Total (%) |
|
|
Location of Participant (n = 33) *COOUTH, Awka General Hospital Onitsha IyiEnu Mission Hospital, Ogidi pNAUTH, Nnewi St Charles Borromeo Hospital, Onithsa |
4 2 9 12 2 |
0 0 1 2 1 |
4 (12.1%) 2 (6.1%) 10(30.3%) 14(42.4%) 3(9.1%) |
|
Total |
29 |
4 |
33 (100%) |
|
Age in Years (n = 33) 20 - 30 Years 31 - 40 Years 41 - 50 Years 51 - 60 Year |
7 16 5 1 |
0 4 0 0 |
7(21.2%) 20(60.6%) 5(15.2%) 1(3.03%) |
|
Mean Age: 35.7 (SD: ± 7.2) Years |
|||
|
Marital Status (n = 33) Single Married |
13 16 |
0 4 |
13 39.4%) 20 60.6%) |
|
What is your primary training in? (n = 30) Medicine Surgery Emergency Medicine |
15 6 5 |
3 0 1 |
18 (60%) 6 (20%) 6 (20%) |
|
Years of Practice (n = 33) 1 - 5 Years 6 - 10 Years 11 - 16 Years 21 Years and Above |
15 9 4 1 |
2 1 1 0 |
17 51.5%) 10 30.3%) 5 (15.1%) 1 (3.03%) |
|
Mean: 6.6 (SD: ±4.4) Years: Modal range of Years of Practice: 1-5 Years |
|||
|
Experience in emergency department? (n = 33) 11 - 15 years 6 - 10 years ≤5 years |
2 7 20 |
0 0 4 |
2 (6.1%) 7 (12.2%) 24 72.7%) |
|
Is your hospital a teaching hospital? (n = 33) Teaching Hospital Non-Teaching Hospital |
16 13 |
2 2 |
18 54.5%) 15 45.5%) |
|
*COOUTH: Chukwuemeka Odumegwu Ojukwu University Teaching Hospital |
|||
Nnamdi Azikiwe University Teaching Hospital
Almost all the respondents 32 (97.0%) have heard about the CT Scan diagnostic technique for up to ten years and virtually all of them 32 (94.0%) stated they have CT machine in their respective hospitals. There responses showed they were equally distributed regarding their training on the radiation doses of medical imaging modalities. The rest of the respondents' awareness about CT scan diagnostic techniques are summarized in table 2.
|
Table 2: Awareness Respondents Towards Use of Computed Tomography. |
|||
|
Variables |
Proportion of Respondents |
||
|
Male |
Female |
Total n(%) |
|
|
Heard of computed tomography (CT)? (n = 33) Yes No |
28 1 |
4 0 |
32 (97%) 1 (30.3%) |
|
How long have you known CT? (n =33) 1-10years 11-20 years 20years and above |
18 9 2 |
2 1 1 |
20(60.6%) 10(30.3%) 3 (9.1%) |
|
Have CT machine in your hospital? (n = 33) Yes No |
28 1 |
3 1 |
31(94%) 2 (6.06%) |
|
How often are your CT scans available? (n=28) Available 24 hours a day, seven days a week Available only during working hours |
16 8 |
2 2 |
18(64.3%) 10(35.7%) |
|
Patients’ emergency visits last year (n = 29) <50,000 50,000-100,000 |
17 8 |
3 1 |
20(69%) 9 (31%) |
|
Were you Trained on specific radiation doses of medical imaging? (n=30) Yes No |
12 14 |
3 1 |
15(50%) 15 50%) |
Most of the respondents showed high level of awareness about the category of patients who should receive medical imaging scan. According to their responses greater proportion of them, 42.6% stated that such procedures are indicated for patients with head injury. Other category of patients indicated were: patients with cardiovascular accidents (CVAs)14.8%, trauma patients 11.1% and patients with neurological defects 9.3%. The results of their awareness responses are summarized below.
|
Table 3: Respondents’ Attitudes Towards Use of Computed Tomography. |
|||
|
|
Proportion of Respondents |
||
|
Variables |
Male |
Female |
Totaln(%) |
|
CT Scan is useful imaging modality? (n=33) |
|
|
|
|
Yes |
29 |
4 |
33 (100%) |
|
How often you refer Head injury patients for CT scan? (n=33) |
|
|
|
|
Always |
12 |
2 |
14 (42.4%) |
|
Most of the time |
13 |
2 |
15 (45.5%) |
|
Sometimes |
4 |
0 |
4 (12.1%) |
|
Do You discuss imaging with patients before requesting it? (n=31) |
|
|
|
|
Always |
17 |
2 |
19 (61.3%) |
|
Most of the time |
8 |
1 |
9 (29%) |
|
Sometimes |
3 |
0 |
3 (9.7%) |
|
Do you refer patients for more of skull x-ray than CT scan? (n=33) |
|
|
|
|
Yes |
6 |
1 |
7 (21.2%) |
|
No |
23 |
3 |
26 (78.8%) |
|
Should head injured patients undergo both X-Ray and CT scan? (n=31) |
|
|
|
|
Yes |
9 |
2 |
11(35.5%) |
|
No |
19 |
1 |
20 (64.5%) |
|
Do you think CT is better than skull x-ray in the examination of head injury? (n=33) |
|
|
|
|
Yes |
28 |
4 |
32(97.0%) |
|
No |
1 |
0 |
1 (3.0%) |
|
Does CT subject the patient to any risks? (n=28) |
|
|
|
|
Yes |
23 |
3 |
26(92.9%) |
|
No |
2 |
0 |
2 (7.1%) |
|
Risk(s) of CT outweigh its benefits? (n=29) |
|
|
|
|
Yes |
12 |
1 |
13(44.8%) |
|
No |
14 |
2 |
16(55.2%) |
|
Do you think this modality should be continued? (n=28) |
|
|
|
|
Yes |
25 |
3 |
28 (100%) |
|
Note: Among the miscellaneous patients included by the respondents were patients with tumours / other malignancies; spinal injury; meningitis; stroke and unconscious and bleeding patients. |
|||
Discussion
The study showed that 29 (87.88%) of the emergency physicians were males and 4 (12.12%) of the emergency physicians were females. It was also seen that 51.5% of the emergency physicians in the various government hospitals fall within 1-5years of practice in these hospitals under study and the remaining 51.57% was shared among the other range of years of practice of the physicians in the various hospitals. In spite of the relative literacy of CT imaging modality and its use shown by the emergency physicians, the study shows that 2 of the emergency physicians (7.1%) don't know that CT scan subjects the patient to some form of risks and also13 of the emergency physicians (44.8%) do not know that the benefits the patients derive from undergoing an examination with this imaging modality outweighs the risk he/she is subject to from this examination. This implies that the level of awareness towards the use of CT in the examination of head injury patients by the sampled population which represents the entire population in the areas of study is high. The study also tries to know what the emergency physicians think about the usefulness of the imaging modality in head injured patients as compared to skull x-ray, it is thus revealed by this study in fig. 13 that all the emergency physicians (100%) are aware that CT is a useful modality and should be used in the examination of head injury. All the emergency physicians were asked whether CT scan is better than the skull x-ray in the examination of head injury and 32 (97.0%) of them stated that CT scan is better that skull X-ray for the management of patients with head injury while 28 of them from the different hospitals stated that CT scan is their imaging modality of choice.
Assessment of Attitude Towards the Use of CT
In spite of the high level of awareness of the emergency physicians towards the use of this imaging modality, their attitude towards the use of this imaging modality (CT) differs greatly among the emergency physicians in the different hospital of employment. The study as revealed in table 2 shows that the emergency physicians from NAUTH and IYIENU (87.9%) refer their head injury patients always and most of the time for CT examination; this is due to the availability of the imaging modality within reach in the department, its ability to delineate intracranial injuries and other diagnostics information that skull x-ray cannot give, its accuracy in diagnosis and management. This is not obtainable in the emergency physicians from the other hospital of employment (COOUTH, St Charles and General Hospital, 12.1% who sometimes refer their patients for CT scan) because of the non-availability, cost and accessibility problems of the equipment.
The study also revealed in table 3 that 26 (78.8%) of the emergency physicians from the different hospitals refer their head injury patients for just CT scan and not for both imaging modality since CT reveals all that skull x-ray can show and even more and thus reducing the risk of excess radiation dose to the patient and also reducing the cost of undergoing two different imaging modalities whereas 11 (35.5%) of the emergency physicians from the different hospitals will refer their patients for both imaging modalities so as to be on a safe side due to either unavailability of CT scan machine, the cost of undergoing a CT scan, and also to serve as a means of comparison. Some of the physicians opt for both imaging procedures to be performed not because they do not know that CT scan can give all the necessary information that is needed for diagnosis but because they think skull x-ray is the first imaging modality, and aids in better visualization of bone fractures to determine the full extent, thus subjecting the patients to excess radiation dose and cost increment. This implies that the attitude of the emergency physicians towards the use of CT in patients with head injury is greatly affected by the non-availability of the machine, the cost of undergoing the investigation and the associated risks involved in using the machine as a diagnostic tool.
Summary and Conclusion
The awareness of emergency physicians towards the use of CT in patients with head injury was assessed. Facts and figures were obtained and their percentages of occurrences were determined. The extent of awareness, the contributing factors to unawareness and the attitude among the sample size population were also probed into. Furthermore, in accordance with the objectives of this study, the results suggests that we may help the emergency physicians with targeted teaching about radiation, the risk and benefits of undergoing CT examination in conjunction with skull x-ray, and also the need to refer patients with head injury for more of CT examination than skull x-ray since CT does present all that skull x-ray can present and even give more diagnostic information. It is therefore urgently needful that the body in whose hands it lies to educate the emergency physicians especially those that refer patients for x-ray examination or CT scan, put all hands on deck, and devise better strategies to teach them on the immediate and late hazards that could arise in the course of over exposing their patients to radiation by requesting them to undergo both imaging modality for screening and diagnosis.
Recommendation
The creation of strong awareness of the usefulness of CT in head injury patients and the need to always adopt this modality in diagnosis is necessary and obligatory in the management and care of patients. Therefore:
1. Appropriate measures to educate the emergency physicians who need more education on the relevance and use of CT together with its associated risk. To achieve this, it is necessary to design broader interventions to target specific group who need to be educated based on this fact.
2. Emergency physicians in various hospitals should adhere to the Canadian CT head rules of that hospital which was proven to have good specificity for predicting intracranial injury and reducing imaging rates as to indicating that suitable for skull x-rays, head CTs, and in-hospital admissions.
Emergency physicians should strongly advocate the intervention of government towards the availability and reduction in cost of using CT machine for scanning patients with head injury for effective health care delivery.
Limitations of The Study
All efforts put to study a good number of emergency physicians proved abortive due to the fact that the number of physicians working at the emergency unit were minimal in number and that some of them were either on annual leave or on outside posting.
Proposed Area of Further Study
Assessment of patients, physicians and radiologist awareness of radiation dose of CT and its possible risks.
References
1. Adeyekun AA, Obi-Egbedi-Ejakpovi EB. 2013. Computerized tomographic patterns in patients with head injury at the university of Benin teaching hospital. Niger J Clin Pract. 16: 19-22. Ref.: https://www.ncbi.nlm.nih.gov/pubmed/23377463
2. Borczukpord SJ. 1995. Predictors of intracranial injury in patients with mild head trauma. Ann Emerg. Med. 25: 731-736. Ref.: https://www.ncbi.nlm.nih.gov/pubmed/7755192
3. Bushberg JT, Siebert JA, Leidholdt EM, et al. 1993. The essential physics of medical imaging Baltimore, Md: Williams & Wilkins.
4. Linda J Carroll, David Cassidy J, Lena Holm. 2004. Methodological issues and research recommendations for mild traumatic brain injury: the WHO collaborating tasks force on mild traumatic brain injury. J Rehabil. 43: 113-125. Ref.: https://go.aws/2RhLju0
5. Computed tomography-definition from the Merriam-webster dictionary. 2009. Retrieved-08-18.
6. Curtis O, Edward H. 2012. Insights Imaging 3: 419-431.
7. Faul M, Xu L, Wald MM, et al. 2010. Traumatic brain injury in the United States: emergency department visits, hospitalizations, and deaths 2002-2006. Atlanta: Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Ref.: https://bit.ly/2uuD0Sz
8. Fischer J, Mathieson C. 2001. The history of Glasgow Coma Scale: Implications for practice. Crit Care Nurs Q. 23: 52-58. Ref.: https://www.ncbi.nlm.nih.gov/pubmed/11852950
9. Fox SH. 1995. CT tube technology. In: Fowlkes JB, eds. Medical CT and ultrasound: current technology and applications. Madison, Wis: Advanced Medical Publishing. 349-377.
10. Gould RG. 1994. CT overview and basics. In: Gould RG, eds. Specification, acceptance testing and quality control of diagnostic x-ray imaging equipment. AAPM Monograph 20. New York, NY: American Institute of Physics. 801-831.
11. Hendee WR, Ritenour R. 1992. Medical imaging physics St Louis, Mo: Mosby.
12. Howlader N, Noone AM, Krapcho M, et al. 2013. SEER Cancer Statistics Review, 1975-2010, National Cancer Institute. Bethesda, MD.
13. Hounsfield GN, 1980. Nobel Award address: computed medical imaging. Med Phys. 7: 283-290. Ref.: https://www.ncbi.nlm.nih.gov/pubmed/6993911
14. Hounsfield GN. 1995. Computerized transverse axial scanning (tomography). I. Description of system: 1973. Br J Radiol. 68: H166-H172. Ref.: https://bit.ly/38pmlPc
15. Temple N, Cortny D, Skora A, et al. 2015. Discipline of Medical Radiation Sciences, J Med Radiat Sci. 62: 122-131.
16. Paul, Marik E, Varon J, et al. 2002. Management of head trauma. 122: 699-711 Ref.: https://www.ncbi.nlm.nih.gov/pubmed/12171853
17. Singh H. 1989. Pattern and distribution of CVA and silent infarcts. J Indian Acad. Forensic Med.11: 23.
18. Stiell IG, Clement CM, Rowe BH, et al. 2005. Comparison of the Canadian CT head rule and the New Orleans criteria in patients with minor head injury. JAMA. 294: 1511-1518. Ref.: https://www.ncbi.nlm.nih.gov/pubmed/16189364
19. Stiell IG, Wells GA, Vandemheen K, et al. 2001. The Canadian CT head rule for patients with minor head injury. Lancet. 5: 1391-1396. Ref.: https://bit.ly/2tKhjxR
20. Stiell IG, Wells GA, Vandemheen K, et al. 1997. Variation in ED use of computer tomography for patients with minor head injury. Ann Emerg Med. 30: 14-22. Ref.: https://bit.ly/2Gg4hej
21. U.S. Food and Drug Administration. 2009. What are the radiation risks from CT. Retrieved July 19, 2013.
22. Wei-Hsiu L, Yung-Hsiao C, Cheng-Ta H, et al. 2011. The Journal of Emergency Medicine. 482-485.
23. Winegar BA, Murillo H, Tantiwongkosi B. 2013. Spectrum of critical findings on complex facial skeleton trauma. Radiographics. 33: 3-19. Ref.: https://bit.ly/36nUkpz
24. Wikipedia.org/emergency_physicians/. 2014.


















