
-
Mail us:
editor@raftpubs.org
Indexing & Abstracting
Full Text
Research ArticleDOI Number : 10.36811/ojgor.2019.110009Article Views : 23Article Downloads : 18
Impact of white poisons in Management of Women with Pcos
Prapurna Chandra Y1*, Amani C2, Shahistha CM2, Sruthi K2, Ayesha SK2 and Sandeep T2
1Department of pharmacology, Andhra University, Visakhapatnam, India
2Rao's college of pharmacy, Nellore, India
*Corresponding Author: Dr. Y. Prapurna chadra M.Pharm Ph.D, Andhra University, Visakhapatnam India, Tel: 9000444948; Email:prapurnachandra@gmail.com
Amani C, Tel: 7981565033; Email: ammujs16@gmail.com
Shahistha CM, Tel: 7842369091; Email: shahisthakhn78@gmail.com
Sruthi K, Tel: 7569825383; Email: ayeshashaik12726@gmail.com
Ayesha SK, Tel: 8801243308; Email: ayeshashaik12726@gmail.com
Sandeep T, Tel: 6281162712; Email: sandeeptatturi199526@gmail.com
Article Information
Aritcle Type: Research Article
Citation: Prapurna Chandra Y, Amani C, Shahistha CM, et al. 2019. Persisting teen age births, a global challenge. O J Gyencol Obset Res. 1: 46-57.
Copyright: This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Copyright © 2019; Prapurna Chandra Y
Publication history:
Received date: 20 November, 2019Accepted date: 29 November, 2019
Published date: 02 December, 2019
Abstract
Introduction: The Poly Cystic Ovaries Syndrome is considered to be most prevalent of all endocrine disorders which women face. It is the leading cause of Infertility in women of child bearing age. The purpose of our study was tocollect data on how many women had symptoms of this syndrome including hirsutism, amenorrhoea, dysmenorrhoea and oligomenorrhoea. Furthermore what was the ratio of women who were aware of this disorder was evaluated.
Methods: Data was collected from Eighty eight women who were either seeking or imparting education in Rao’s college of pharmacy. A small portion of our subjects were educated house wives. Subjects were inquired through survey forms of above mentioned symptoms.
Results: The collected data was then interpreted to find the prevalence of above mentioned symptoms and awareness about PCOS. 17% of 88 women had Acne & Hirsutism. Regarding menstruation 18.1% had some sort of irregularity with hirsutism and 30.6% had menstrual irregularity with acne. 13.6% had acne, hirsutism and menstrual irregularity. 17.4% of women are till consuming the 5 white poisons out of 88 women.
Discussion: The results show that the level of awareness about dietary white poisons in the study population is very low, even in the participants who are literates, in this study we concluded that dietary white poisons may play essential role in management of weight loss, and helps to reduce the symptoms which is very common in the PCOS. We have also observed that by avoiding & replacing the white poisons such as refined rice, wheat, high sugar and salts and pasteurized milk, helps to regulate the biochemical hormones like Androgen and Progesterone which, abnormalities are very common in the PCOS. Hence we conclude that management of diet helps in the management of PCOS in the study population.
Keywords: Ovaries Syndrome; Hirsutism; Oligomenorrhoea; Ultrasonography
Introduction
Poly Cystic Ovarian Syndrome (PCOS) is the most widely recognized and complex endocrinal disorder influencing females of child bearing age [1]. It is also known as hyper androgenic anovulation and stein-Leventhal syndrome [2].
Now a day’s PCOS is perceived to be a metabolic disorder [3] and It is discriminated by prolonged anovulation, hyper-androgenism, infertility and often Women with this syndrome have been noticed to be hyperinsulinemic [4]. Currently Rolterdam criteria is preferred for diagnosing PCOS which states that for determining the PCOS with the accompanying signs such as anovulation/oligo ovulation, hyper-androgenemia and appearance of polycystic ovaries on ultrasound [5].
PCOS is a heterogenic disorder with intermediate aetiology and is described by androgen excess and polycystic ovaries. Ovulatory dysfunction is the most important clinical aspect observed in PCOS [6]. It is considered as a multi-organ disorder as it can impact adrenal and sex hormones along with ACTH gonadotropins and development hormone [7].
According to Fauser B.C.J.M studies 6-15% infertility is due to PCOS [8]. The incidence of PCOS can be as high as 30% in women with insignificant amenorrhea, 15% in women with oligomenorrhea and 90% in women with hirsutism [9].
Patients with PCOS are at risk of diabetes mellitus as they suffer from insulin resistance besides the symptoms of abdominal obesity in addition to increase secretion of interleukins, chemokines and adipokines (because of body’s inflammatory state) [10]. The hallmark of this disease can be described into clinical, endocrine and metabolic. The clinical features are abnormal menstrual, acne, hirsutism, alopecia, anovulation, infertility and miscarriages. The endocrine features are increased levels of androgens leutinizing hormone and prolactin. The metabolic perspective of this disorder is insulin resistance, obesity, lipid abnormalities and as increased risk of impaired glucose tolerance which can lead to Type 2 Diabetes. And further more hazard for cardiovascular disease and endometrial carcinoma [11,12].
Life style interventions are the first-line treatment for PCOS, especially when it is accompanied by obesity. This suggested priority is based on the fact that reduction of central fat ameliorates the PCOS phenotypes, inter alia improved cyclicity and resumption of ovulation [13]. Also, weight loss improves the status of cardiovascular risk factors accompanied by a decreased intima media thickness [14].
According to the literature, dietary management is the primary choice to treat the PCOS and many studies described that increased intake of five white poisons such as pasteurized milk, refinedsalt, refinedrice, refinedsugar, and white flour.
The process of pasteurization keeps the milk good for a longer period but harms its nutritive value. It removes enzymes, vit-A, B12 and C beneficial bacteria &calcium. Calcium works with vit-D which is vital to growth &health of children as well as improving immune system. Considering all these facts we should avoid consuming pasteurised milk.
Salt makes body hold on to water if you eat too much salt. The extra water stored in your body increase your B.P.
The process of refining rice beats to the removal of outer layer, germ &endosperm only these layers contains starch in huge quantity which can increase blood sugar to a great extent.
Refined sugar can cause insulin resistance, a stepping stone towards metabolic syndrome & diabetes. Insulin is a very important hormone in the body. It allows glucose to enter cells from the blood stream &tells the cell start burning glucose instead of fats.
Maida Known as white poison. We are consuming it in the form of bread at our home and market or food joints in the form of fast food. During processing of maida from wheat endosperm, germ and bran and nutrients are removed, which is very crucial for digestion. As a result, our body get depleted of vitamins &minerals. High intake of the above said white poisons in diet leads to Obesity, Diabetes, Hormonal imbalance, Cancer [15].
Obesity is a common finding in PCOS and aggrevates many of its reproductive and metabolic features. The relationship between PCOS and obesity is complex, not well understood and most likely involves interaction of genetic and environmental factors [16]. In this study we aimed to evaluate the effect of dietary white poisons in women with PCOS and to evaluate the knowledge of women about diet and obesity.
Women with PCOS had a greater risk of overweight, obesity and central obesity although our findings support a positive association between obesity and PCOS, our conclusion are limited by the significant heterogeneity between studies and further studies are now required to determine the sources of these heterogeneity. Clinical management of PCOS should include the prevention and management of overweight and obesity [17].
The pcos is a metabolic disease which has unfavorable effects on lipid profile, carbohydrate metabolism and cardiovascular risk parameters. It has been shown that some drugs which are used in treatment of some pcos also unfavourable effects on these parameters. Therefore, the metabolic effects of drugs should be considered in treatment [18].
The Metaanalysis showed a twofold risk of arterial disease for patients with pcos in respect to women without pcos. BMI modification did not impact these findings, suggesting the expanded hazard for cardiovascular event in the pcos isn’t totally identified with higher BMI in patients with pcos [19].
Aim and Objective
• To study and evaluate the effect of dietary white poisons in women with pcos.
• To evaluate the knowledge of women about diet and obesity.
• To evaluate the effect of patient counselling in study population
Methodology
This study was conducted in Nellore which is a city of India, a country situated in South Asia [20]. This research study was approved by Institutional Ethics Committee of RaosCollege of Pharmacy, Nellore. In this study, 88 female, Pre-Menopausal women with PCOS were recruited into the study. All subjects were given informed consent before participating in the study. Participants who were diagnosed of PCOS, according to the Rotterdam consensus by two of the following three criteria 1) Menstrual irregularity (cycle length < 26 days or > 31 days).2) Clinical (Hirsutism or biochemical hyper androgenize (free androgen index >5.4 or testosterone >1.4 mmol/L.3) Pasitive ultrasound presentation of PCOS by trans vaginal smear. Women with pregnancy, breast feeding and those who are in use of oral contraceptives and hormonal treatment, those who are using insulin sensitizing agents are excluded from the study.
All the subjects documented their menstrual cycle throughout the study duration, weight change Biochemical measurements and symptoms such as acne, Hisutism were also documented. All study participants were counselled about the dietary white poisons and their complications and suggested the how to avoid those poisons and given alternatives to replace the white poisons, and all study participants were followed up throughout the study period. At the end of the study all participants were again interviewed and collected the data and disseminated.
Statistical evaluation
Data was presented as Mean ± SEM, results are presented for 88 subjects, two tailed statistical analysis was performed using SPSS for windows 10.0 software (SPSS Inc, Chicago, USA.)
PRE QUESTIONARIES
PATIEN INFORMATION (DEMOGRAPHIC DETAILS):
Name:
Date of birth:
Age:
Height:
Weight:
Phone no:
Education qualification:
Occupation:
Current status:
1) What are the primary reasons for consultation check those that apply?
Lose weight Irregular periods
Infertility Relieve symptoms of PCOS others
2) Do you have any other significant medical history such as high B.P, Diabetic, Thyroid etc.?
3) If you are diabetic. Are you insulin resistant?
4) What are your symptoms?
Irregular periods Mood swings
Hair loss Difficulty sleeping
Excessive hair growth Skin issues
5) What medications are you on and how long have you been on them for?
6) Are you taking any vitamins/mineral supplements? please list.
7) Are you exercising on a regular basis? If so, please describe what activity, how many times a week & for how long?
8) If you are not exercising, why not?
9) Do your family members (parents, siblings) have weight problems?
DIET
10) Give an idea of what kind of diets you have tired (low fat, low carbohydrates etc.)
11) Did you have success with diet?
Yes No
12) Where do you feel that some of your problem’s areas might be? Check all those that apply?
Emotional eaters Large portions
Crave sweets Crave others crabs
Excessive fat intake Eat out alot
Too few calories Inadequate exercise
13) Please check off which of the following foods you would eat?
|
DRINKS |
SWEETNERS |
FLOURS |
HIGH SALTS |
LOW SALTS |
RICE |
|
|
Tea |
Sugar |
Wheat flour |
Pickles |
Fruits |
Parboiled rice |
|
|
Coffee |
Honey |
Maida flour |
Chips |
Vegetables |
Polished rice |
|
|
Almond milk |
Jiggery |
Rice flour |
Corn snacks |
Eggs |
Brown rice |
|
|
Pasteurized milk |
Candy |
|
Prawns |
Cakes& cookies |
|
|
|
Yogurts |
|
|
Soups |
|
|
14) List several choices for each meal/snack as well as the time that you might eat it?
Breakfast:
Snack:
Lunch:
Snack:
Dinner:
Snack:
15) I crave carbohydrates and sugars
Yes No
16) I have always had difficulty with losing weight?
Yes No
17) I have or had problems in the past acne
Yes No
18) My periods last longer than 35 days
Yes No
19) My periods are unpredictable
Yes No
20) My periods last longer than a week
Yes No
21) My periods are very heavy or prolonged
Yes No
22) I have with excessive facial hair
Yes No
23) I have symptoms of hypoglycemia
Yes No
24) I feel extremely hungry, irritable, sleepy or fatigued after eating sweets
Yes No
25) I have a family history of diabetes
Yes No
26) I have noticed skin color or pigmentation changes
Yes No
27) I have history of high blood pressure
Yes No
28) I have difficulties getting pregnancy
Yes No
29) I have PMS symptoms
Yes No
30) My acne is worse at different times of my cycle
Yes No
Post Questionaries
POST INTERVENTION QUESTIONARIES
Name:
Age :
Date of birth:
Weight: BMI:
Occupation:
Education:
1. Are you on regular periods after changing the diet?
¨ Yes ¨ No
2. Has your androgen levels are normal?
3. Have you seen changes in your symptoms after changing diet and starting exercise?
¨ Yes ¨ No
4. Have you been working out every day for about an hour?
¨ Yes ¨ No
5. Please choose, which type of food did you cut down/out from your diet?
Polished rice
Maida
Refined sugar
Refined salt
Pasteurized milk
6. Comment how did you replaced above said white poisons in your diet?
Polished rice: ______________________________________________
Maida: ___________________________________________________
Refined sugar: _____________________________________________
Refined salt: _______________________________________________
Pasteurized milk: ___________________________________________
7. Do you think that the lifestyle changes have reduced your PCOS symptoms?
¨ Yes ¨ No
If Yes, please mention choose, what type of modification did you practiced.
¨ Regular Exercise ¨ Yoga
¨ Diet modification ¨ Meditation
8. Are your insulin level are in normal values date when last test performed?
¨ Yes ¨ No`
9. Are your thyroid level in normal values date when last test performed?
¨ Yes ¨ No
10. Have your hirsutism is reduced?
¨ Yes ¨ No ¨ N/A
11. Have your acne is reduced?
¨ Yes ¨ No ¨ N/A
12. Has your PMS symptoms are relieved like back pain, stomach ache, etc.
¨ Yes ¨ No ¨ N/A
13. Are your Progesterone and estrogen are in normal level?
¨ Yes ¨ No ¨ N/A
14. Are you taking Fibers daily that promotes estrogen metabolism. check out Fibers
Beans
Leafy vegetables
Apples
Whole grains
15.what has helped you in dealing with PCOS?
Results
Our sample size was 88 Rural women from the age group of 15-45yrs.out of this88, 11 are under age group of15-20 and 25 are in the age group of 21-25,32 are in age group of 26-30,15 are in the age group of 31-35, 5 are under 36-45.
|
Table1: Distribution of age group in the study population. |
||
|
Z |
No.of.Patients (n=88) |
Percentage (%) |
|
15-20 |
11 |
12.5 |
|
21-25 |
25 |
28.4 |
|
26-30 |
32 |
36.3 |
|
31-35 |
15 |
17 |
|
36-45 |
5 |
5.6 |
|
Total |
88 |
100 |
|
Out of this 88 womens 14(15.9%) are students and 49(55.6%) are housewifes, 25(28.4) areworking womens. |
||
Pre-study interventions
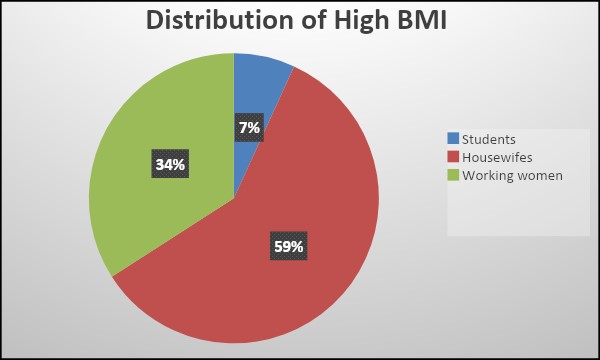
In this Study, as shown in Figure1. Out of 88 participants 16 % are students, 28% are working women and 56 % are House wives, and according to the BMI scale, 50 % of the population were fallen under overweight as depicted in Table 2. Out of this 59 %, 34 % and 7% are from House wives, working women and students respectively as shown in Figure 2.
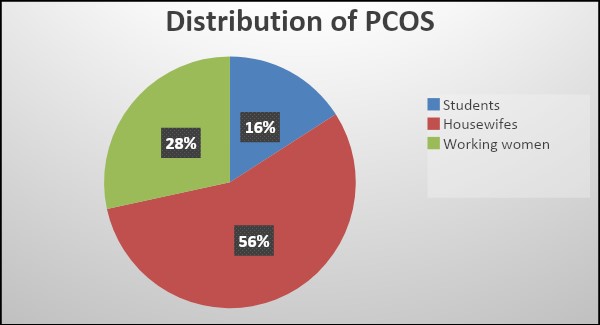
Figure1: Distribution of PCOS in women.
|
Table 2: Distribution of BMI based on occupation. |
|||||
|
Pre- BMI |
Students |
Housewife’s |
Working women |
Total |
Percentage (%) |
|
Under weight |
2 |
0 |
2 |
4 |
4.5 |
|
Normal weight |
9 |
23 |
8 |
40 |
45.4 |
|
overweight |
3 |
26 |
15 |
44 |
50 |
According to the questionnaire 45 participants are consuming dietary white poisons daily, which is 51.13 % of the whole population.
The major common symptoms were observed in the study participants is Acne, Hirsutism and Irregular periods, and incidence of these symptoms are given in Table 3.
|
Table 3: incidence of symptoms in the participants |
||
|
Pre symptoms |
No. of patients |
Percentage (%) |
|
Acne+Hirsutism |
18 |
20.4 |
|
Acne +IRP |
37 |
42 |
|
Hirsutism+IRP |
19 |
21.5 |
|
Acne+Hirsutism+IRP |
15 |
17 |
Pre –intervention bio chemical hormones such as Androgen and Progesterone was estimated and observed as abnormal levels in majority of the study participants i.e.,89.7 %, results are depicted in table 4.
|
Table 4: Distribution based on hormone levels |
||||
|
Pre-Hormones |
Normal Range |
Percentage (%) |
Abnormal (High level) |
Percentage (%) |
|
Androgen |
9 |
10.2 |
79 |
89.7 |
|
Progesterone |
9 |
10.2 |
79 |
89.7 |
Post-intervention
After pre study questionnaire, the study participants are suggested with diet plan and given counselling to create awareness among the study participants to avoid white poisons and replace them with balanced and organic food items, and ensured to maintained modified diet plan with continuous follow-up for 4 Months, after the study period, the study team again interviewed the participants for post-intervention parameters.
After post study intervention High BMI population are reduced to from 50 % to 36.3% due to modification in diet, as depicted in table 5.
|
Table 5: Post-study distribution of BMI based on occupation. |
|||||
|
Post-BMI |
Students |
House wives |
Working Women |
Total |
Percentage |
|
Under Weight |
2 |
2 |
1 |
5 |
5.6 |
|
Normal Weight |
11 |
27 |
13 |
51 |
57.9 |
|
Over Weight |
1 |
20 |
11 |
32 |
36.3 |
Table 6, described that post study symptomology of the study population, and also observed reduced incidence of symptoms compared to pre-study.
|
Table 6: Comparison of symptom of PCOS (Pre& Post intervention). |
|||
|
Symptoms |
Pre-Intervention |
Post-Intervention |
P value |
|
Acne+Hirsutism |
18 |
15 |
0.00 |
|
Acne +IRP |
37 |
27 |
0.05 |
|
Hirsutism+IRP |
19 |
16 |
0.00 |
|
Acne+Hirsutism+IRP |
15 |
12 |
0.00 |
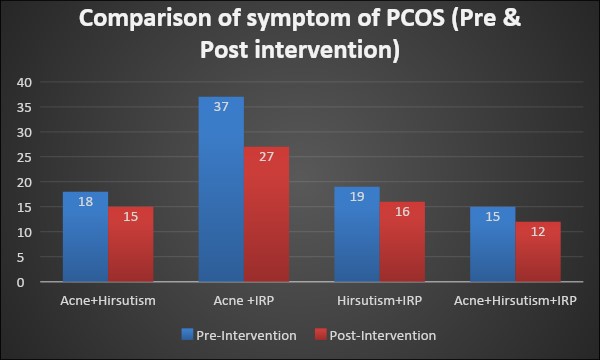
Figure 3: Comparison of symptom of PCOS (Pre & Post intervention).
Post –intervention of bio chemical hormones was also estimated and observed significant reduction in the levels of androgen and Progesterone as shown in figure 4.
|
Table 7: Pre &Post study distribution of Biochemical hormones. |
|||||
|
Hormones |
Pre-study |
Post study |
P value |
||
|
Normal Range |
Abnormal (High level) |
Normal Range |
Abnormal (High level) |
||
|
Androgen |
9 (10.2) |
79 (89.7) |
67(76.13) |
21 (23.86) |
0.01 |
|
Progesterone |
9 (10.2) |
79 (89.7) |
73 (82.95) |
15 (17.04) |
0.01 |
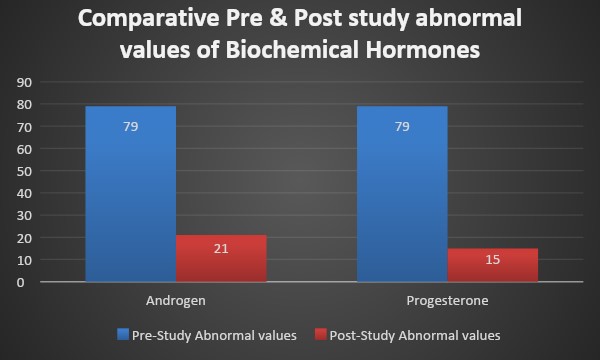
Figure 4: Comparative Pre & Post study abnormal values of Biochemical hormones.
Discussion
Total number of people who participated in this study was 88 women. In these 88 rural women, only 25(28.4%) educated women had heard about this effect of white poisons. The numbers concluded that 28.4% of women in our study knew about this effect of white poisons. But if we exclude females who are educated, we can say that much fewer women had any kind of knowledge regarding this white poison issue.
Out of these 88 women, 45(51.13%) women are consuming the five white poisons. In answer to question whether there are women who had replaced the five white poisons only 30(34.09%) women responded positively.
A rough data on symptoms was also collected which suggested that majority of women in our study suffered from symptoms including acne, hirsutism and irregular periods. 18 women reported to have acne and hirsutism, 37 women reported to have acne and irregular periods while 19 women reported to have hirsutism and irregular periods, 15 women reported that they have acne, hirsutism and irregular periods.
On the whole 79(89.7%) out of total 88 women reported that they have abnormal levels of androgen and progesterone levels. Weight loss among overweight women has been shown to improve reproductive outcomes by reducing sugar intake [21]. Clark et al. found that even a small weight loss in an ovulatory obese infertile women resulted in improvement in ovulation, pregnancy rate and outcome [22].
Conclusion
The results show that the level of awareness about dietary white poisons in the study population is very low, even in the participants who are literates, in this study we concluded that dietary white poisons may play essential role in management of weight loss, and helps to reduce the symptoms which are very common in the PCOS. We have also observed that by avoiding & replacing the white poisons such as refined rice, wheat, high sugar and salts and pasteurized milk, helps to regulate the biochemical hormones like Androgen and Progesterone which, abnormalities are very common in the PCOS. Hence, we conclude that management of diet helps in the management of PCOS in the study population.
Acknowledgement
We would like to avail this opportunity to express deep sense of gratitude and heartfelt thanks to our revered guide Mr.Prapurna Chandra.Y.M.Pharm Ph.D department of pharmacology, Raos college of pharmacy, Nellore, for his unflinching support, valuable suggestions and for sharing his experience with us during the entire course.
References
1. Abboh DH, Dumesic da franks. 2002. Review developmental origin of polycystics ovary syndrome. J.Endocrinol. 174: 1-5.
2. USMLE-Rx.Medlu learning llc .2014.
3. Norman RJ, WU R, stankiewicz M. 2004. Polycystic ovary syndrome. 180: 132-137. Ref.: https://bit.ly/2KYUps2
4. loverro G, vicinoM,lorussu F ,VimercatiA,Greco P. et al. 2001. Polycystic ovary syndrome: relationship between insulin sensitivity,sex hormone levels and ovarian stromal blood flow.Gynecol Endocrinol. 15: 142-149. Ref.: https://bit.ly/35EbgID
5. Shroff R, Syrop C, Davis W, et al. 2007. risk of metabolic complications in the new pcos phenotypes based on Rotterdam criteria. Fertil Steril. 88: 1389-1395. Ref.: https://bit.ly/2OV4dEA
6. Fr DD, Tarlatzis R. 2004. Consensus on diagnostic criteria and longterm health risk related to polycystic ovary syndrome. Fertil Steril. 81: 19-25.
7. Radosh lee. 2009. Drug treatments for polycystic ovary syndrome American family physician, Drug treatment for polycystic ovary syndrome. 79: 671-676. Ref.: https://bit.ly/2OsPce9
8. Fauser BC, tarlatzis BC, Rebar RW, et al. 2012. consensus on womens health aspect of polycystic ovary syndrome.Fertil Steril. 97: 28e25- 28e38. Ref.: https://bit.ly/33uTN3Q
9. Boomsma CM, Fauser BC, Macklon NS. 2008. Pregnancy complications in women with polycystic ovary syndrome.seminreprod med. 26: 72-84. Ref.: https://bit.ly/2OQd9eC
10. Glintborg D, Andersen M. 2010. An update on pathogenesis, inflammation and metabolism in hirsutism and pcos.Gynecol Endocrinol. 26: 281-296. Ref.: https://bit.ly/2OP0gBm
11. Tasoula, Tsilchorozidou, Overton C, et al. 2004. The pathophysiology of polycystic ovary syndrome. ClinEndocrinol(OXf). 60: 1-17. Ref.: https://bit.ly/34q8TJm
12. Carmina E. 2009. Cardiovascular risk and events in polycystic ovarysyndrome. climactric.12: 22-25. Ref.: https://bit.ly/2XVkEoo
13. Kuchenbecker WKH, Groen H, Van Asselt SJ, et al. 2011. In women with polycystic ovary syndrome and obesity, loss of intra abdominal fat is associated with resumption of ovulation. Hum Reprod.26: 2505-2512. Ref.: https://bit.ly/2OP1v3u
14. Lass N, Kleber M, Winkel K, et al. 2011. Effect of life style intervention on features of polycystic ovary syndrome, and intima-media thickness in obese adolescent girls. J ClinEndocrinol Metab. 96: 3533-3540. Ref.: https://bit.ly/2QZkYBo
15. 5 white poisons that we eat unknowingly-practo.http://www.practo.com > post.
16. Susan Sam, MD. 2007. Obesity and polycystic ovary syndrome. 3: 69-73.
17. Lim SS, Davis MJ, Norman RJ, et al. 2012. Over weight, obesity and central obesity in women with polycystic ovary syndrome: A systematic review and meta analysis. 18: 618-637. Ref.: https://bit.ly/37Diy10
18. MeliaKarakose, ermancakal, tuncaydelibasi. 2013. metabolic effects of drugs used for treatment of polycystic ovary syndrome. 14: 168-173. Ref.: https://bit.ly/2qJhQyS
19. Degroot PCM, Dekkers OM, Romijn JA, et al. 2011. pcos, coronary heart disease, stroke and influence of obesity:a systematic review and meta , analysis. 17: 495-500. Ref.: https://bit.ly/34wX7Ne
20. Somia Gul, Syeda Adeeba Zahid, Almas Ansari. 2014. pcos:symptoms and awareness in urban pakisthani women. 2: 356-360. Ref.: https://bit.ly/2XYkuwD
21. ZeynepOzcan Dag, BernaDilbaz. 2015. Impact of obesity on infertility in women. Ref.: https://bit.ly/2OSy7Jz
22. Clark AM, Thornley B, Tomlinson L, et al. 1998. Weight loss in obese infertile women results in improvement in reproductive outcome for all forms of fertility treatment. 13: 1502-1505. Ref.: https://bit.ly/2L0ME4W


















