
-
Mail us:
editor@raftpubs.org
Indexing & Abstracting
Full Text
Case ReportDOI Number : 10.36811/ojdoh.2020.110005Article Views : 12Article Downloads : 117
Root-end restoration using MTA against the intractable cases of root canal treatment
KITAJIMA Kayoko1, ARAI Kyoko1, YOKOSUKA Takashi2, SATOH Tomonori1,2, KITANO Yoshie1, ASAHINA Takeo1, MIYOSHI Toshiroh1 and IGARASHI Masaru3
1Department of Endodontics, School of Life Dentistry at Niigata, The Nippon Dental University, Japan
2Comprehensive Dental Care, The Nippon Dental University Niigata Hospital, Japan
3Department of Endodontics, School of Life Dentistry at Tokyo, The Nippon Dental University, Japan
*Corresponding Author: KITAJIMA Kayoko, Department of Endodontics, School of Life Dentistry at Niigata, The Nippon Dental University,1-8 Hamaura-cho, Chuo-ku, Niigata, Niigata 951-8580, Japan, Tel: +81-25-211-8171; Fax: +81-25-267-1795; Email: kitajima@ngt.ndu.ac.jp
Article Information
Aritcle Type: Case Report
Citation: KITAJIMA Kayoko, ARAI Kyoko, YOKOSUKA Takashi, et al. 2020.Root-end restoration using MTA against the intractable cases of root canal treatment. Open J Dent Oral Health.2: 01-07.
Copyright: This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Copyright © 2020; KITAJIMA Kayoko
Publication history:
Received date: 17 March, 2020Accepted date: 23 March, 2020
Published date: 25 March, 2020
Abstract
Root-end restoration using Mineral Trioxide Aggregate (MTA) was performed on two patients who received root canal treatment but had poor progress. In one case, a large amount of Calcium hydroxide(Ca (OH)2), a intracanal medicament, escaped from a wide-open apex, stagnated around the tooth root, and the apical lesion did not disappear. The other case is a case where the root canal at the apical part has a complicated anatomical form, the root canal cannot be tightly packed, and the apical lesion has not disappeared. Root-end restoration using MTA was performed on these two cases, and improvement of the lesion was confirmed. From these results, it was shown that Root-end restoration using MTA is effective for patients with poor prognosis of root canal treatment for which the apical portion cannot be tightly packed for various reasons.
Keywords: Mineral Trioxide Aggregate; MTA;Root-end restoration
Introduction
Mineral Trioxide Aggregate (MTA) is a general material for endodontic treatment and is indicated widely as perforation repair, apexification, pulp capping or root-end filling[1]. At present, the adaptation of MTA in Japan is restricted only to direct pulp capping, and it does not accept to root canal filling, restoration of external resorption, retro filling and closing of perforationon the insured coverage. At our university, it is used only in the example of a patient giving informed consent, based on recognition from Ethical Review Board. This study reports two clinical cases with informed consent. Although the prognosis was poor with normal root canal treatment, root-end restoration using MTA was performed, and these two cases followed a favorable healing process.
Case reports
Case 1: A 25-year-old male was referred to an endodontic clinic from a pediatric clinic for treatment of external resorption of upper left central incisor tooth. The tooth was replanted for luxation by a traffic accident when the patient was 9 years old, and external root resorption was revealed at 24 years old?Figure 1). The root canal treatment was started in the pediatric clinic; however, the prognosis was not preferable because of the over extension of calcium hydroxide paste?Figure 2). The retreatment was referred to our clinicafter 10 months and was tried by a common procedure?Figure 3). Finally, the retro filling with MTA was applied to the cut root end cavity (Figure 4,5). Thirteen months later?Figure 6), the apical healing was confirmed.

Figure 1: Xray image when patient visited pediatric clinic.

Figure 2: Xray image when patient was treated at the pediatric clinic.

Figure 3: Xray image after retreatment and root canal filling.

Figure 4: Oral view of root end cavity.

Figure 5: Xray image after root-end restoration using MTA.

Figure 6: Xray image after thirteen months of the root-end restoration using MTA.
Case 2: A 35-year-old male patient visited to get a second opinion concerning his lower right first premolar. The mandibular first premolar was treated 5 years ago because of dental caries by a general dentist, and the pulp extirpation was performed. The sinus tract appeared on the apical gingiva after three years. The 3D image by cone beam CT showed the apical periodontitis with the defect of buccal cortical bone?Figure 7). The dental X-ray showed the wide root apex of the involved tooth and divided roots canal were doubted.?Figure 8? Since the retreatment was difficult for the anatomical problem, root-end restoration was carried out with MTA?Figure 9,10). Patient was followed up after oneand ten months later?Figure 11,12? the apical lesion disappeared, and the good prognosis was confirmed.
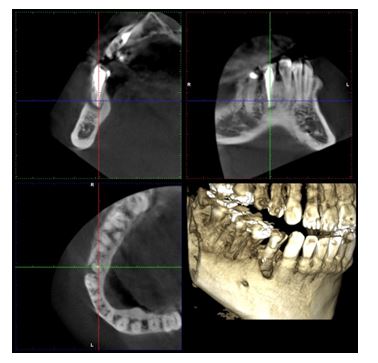
Figure 7: 3D images when patient visited general dentist.

Figure 8: Xray image when patient visited department of endodontics.

Figure 9: Oral view of rootend cavity.
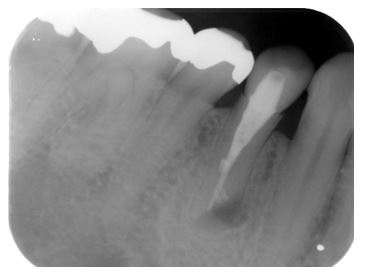
Figure 10: Xray image after root-end restoration using MTA.

Figure 11: Xray image after one month of the root-end restoration using MTA.
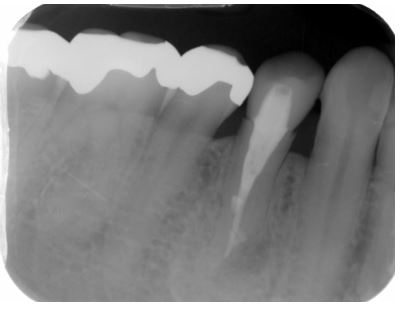
Figure 12: Xray image after ten months of the root-end restoration using MTA.
Discussion
In the event that the root canal system and periodontal tissue are accidentally transported, a sealant is used to protect the teeth. As its material, gutta-percha, polycarboxylic acid cement, zinc phosphate cement, zinc oxide eugenol cement, IRM cement, EBA cement, glass ionomer cement, composite resin and the like have been used. However, these have not always been sufficient as long-term tight-sealing materials. It is considered that sufficient drying of the adhesive tooth surface is indispensable for these to contribute to the tight sealing. However, excessive drying causes great damage to cells on the root surface. MTA was first developed at Loma Linda University in 1993 as a hardened hydraulic cement. That is, it is said that MTA is cured by contact with moisture and maintains a stable state in water after curing [2]. The blockade of MTA is higher than that of amalgam and SuperEBA [3-12], and it is superior in the stain leak test [3,4], bacterial leak test [5], and endotoxin leak test[6]. The suitability of the margin is better than amalgam, IRM and SuperEBA [3]. In addition, antibacterial effects have been confirmed against some resident bacteria in the oral cavity [13]. The toxicity of MTA is lower than that of IRM and SuperEBA [14] in radioactive chromium emission measurement tests, and it is reported that it has high biocompatibility [7,15-18]. Histological studies using amalgam and MTA to reverse the root canal filling and root bifurcation in dogs [8] and reverse root canal filling of monkey teeth [12] showed that MTA has less inflammation of surrounding tissues and is favourable. A long healing process was observed [11-13]. Cementations addition of MTA surface layer after a long period of time, which was not seen with amalgam, was confirmed [14,15]. These results suggest that MTA is effective as an inverted root canal filler. Many subsequent reports have revealed that MTA is an antibacterial, antifungal, biologically active, and highly biocompatible material with high blockade [2]. In this case, when MTA was applied to patients with poor prognosis of root canal treatment, the apical X-ray transmission image disappeared, and good results were obtained. This is considered to be due to the fact that calcium hydroxide is formed in MTA [19-22] and it has the ability to induce hard tissue [23,24]. MTA has been considered as a promising material for root canal fillings, inverted root canal fillings, perforation sealants, pulp capping materials, pulpotomy materials, immature teeth and necrotic pulp teeth. It is noted that the mechanism of action of MTA is that hydroxyapatite crystals are added to MTA when it comes into contact with tissue fluid and can serve as a starting point for calcified tissue formation [25-28], and its suitability as a sealant has been evaluated.From this case report, it was found that the application of MTA as a reverse root canal filling material for surgical endodontic treatment was favourable for patients with a poor prognosis of root canal treatment. The usefulness was suggested.It has been pointed out that the MTA curing time is long. There is a possibility of discoloration, and it is expensive. However, a white MTA that eliminates the mixture, causing discoloration was developed. And the curing time was shortened.MTA development is also underway.It is expected that the indications will be expanded by further improving the adhesiveness in the future.
Conclusion
The root-end restoration with MTA showed the postoperative proper apical healing and MTA is useful endodontic materials for root end surgery.
The Ethics Committee has granted the permission (ECNG-H-41) based on the studies of the foreign countries.
References
1. Parirokh M, Torabinjad M. 2010. Mineral trioxide aggregate; a comprehensive literature review - Part ?: Clinical applications, drawbacks, and mechanism of action. J of Endod. 36: 400-413. Ref.: https://www.ncbi.nlm.nih.gov/pubmed/20171353
2. Parirokh M, Torabinjad M. 2010. Mineral trioxide aggregate; a comprehensive literature review - Part ?: Chemical, physical, and antibacterial properties. J of Endod. 36: 16-27. Ref.: https://www.ncbi.nlm.nih.gov/pubmed/20003930
3. Torabinjad M, Watson TF, Pitt Ford TR. 1993. The sealing ability of a mineral trioxide aggregate as a retrograde root filling material. J of Endod. 19: 591-595. Ref.: https://bit.ly/3dgPFuo
4. Higa RK, Torabinjad M, Mckendry DJ, et al. 1994. The effect of strage time on the degree of dye leakage of root-end filling materials. Int Endod J. 27: 252-256. Ref.: https://www.ncbi.nlm.nih.gov/pubmed/7814137
5. Torabinjad M, Falah R, Kettering JD, et al.1995.Bacterial leakage of mineral trioxide aggregate as a root end filling material. J of Endod. 21: 109-112. Ref.: https://bit.ly/2Uncsw5
6. Tang HM, Torabinjad M, Kettering JD. 2001. Leakage evaluation of end filling materials using endotoxin. J of Endod. 28: 5-7. Ref.: https://www.ncbi.nlm.nih.gov/pubmed/11806652
7. Parirokh M, Torabinjad M. 2010. Mineral trioxide aggregate; a comprehensive literaturereview - Part ?:Leakage and biocompatibility investigations. J Endod. 36: 190-202. Ref.: https://www.ncbi.nlm.nih.gov/pubmed/20113774
8. Torabinjad M, Hong CU, Lee SJ, et al.1995. Investigation of mineral trioxide aggregate for root filling in dogs. J of Endod. 21: 603-608. Ref.: https://www.ncbi.nlm.nih.gov/pubmed/8596081
9. Torabinjad M, Hong CU, Pitt Ford TR. 1995. Physical properties of new root end filling material. J of Endod. 21: 349-353. Ref.: https://bit.ly/2vHhhYM
10. Torabinjad M, Wilder Smith P, Pitt Ford TR. 1995. Comparative investigation of marginal adaptation of mineral trioxide aggregate and other commonly used root end filling materials. J of Endod. 21: 295-299. Ref.: https://www.ncbi.nlm.nih.gov/pubmed/7673836
11. Pitt Ford TR, Torabinjad M, Hong CU, et al. 1995. Use of mineral trioxide aggregate for repaire of furcal perforations. Oral Surg. 79: 756-763. Ref.: https://bit.ly/39a9nop
12. Torabinjad M, Pitt Ford TR, Mckendry DJ, et al.1997. Histologic assessment of MTA as root end filling in monkeys. J of Endod. 23: 225-228. Ref.: https://www.ncbi.nlm.nih.gov/pubmed/9594770
13. Torabinjad M, Hong CU, Pitt Ford TR, et al. 1995.Antibacteria effect of some root filling materials. J of Endod. 21: 403-406. Ref.: https://bit.ly/3b7gxey
14. Torabinjad M, Hong CU, Pitt Ford TR, et al. 1995. Cytotoxicity of four root end filling materials. J of Endod. 21: 489-492. Ref.: https://www.ncbi.nlm.nih.gov/pubmed/8596067
15. Torabinjad M, Hong CU, Pitt Ford TR. 1995.Tissue reaction to implanted SuperEBA and mineral trioxide aggregate in the mandibles guinea pigs: A preliminary report. J of Endod. 21: 569-571. Ref.: https://bit.ly/3dkzwUX
16. Sarkar NK, Caidedo R, Tirwik P, et al. 2005. Physicochemical basis of the biologic properties of mineral trioxide aggregate. J Endod. 31: 97-100. Ref.: https://www.ncbi.nlm.nih.gov/pubmed/15671817
17. Camilleri J, Pitt Ford TR. 2006. Mineral Trioxide Aggrerate: a review of the constituents and biological properties of the material. Int Endod J. 38: 747-754. Ref.: https://www.ncbi.nlm.nih.gov/pubmed/16948659
18. Roberts HW, Toth JM, Berzins DW, et al. 2008. Mineral trioxide aggregate material used in endodontic treatment: a review of the literature. Dent Mater. 24: 149-164. Ref.: https://bit.ly/3abubNB
19. Bozeman TB, Lemon RR, Eleazer PD. 2006. Elemental analysis of crystal precipitate from gray and white MTA. J of Endod. 32: 425-428. Ref.: https://www.ncbi.nlm.nih.gov/pubmed/16631841
20. Tay FR, Pashley DH, Rueggeberg FA, et al. 2007. Calcium Phosphate phase transformation produced by the interaction of the portland cement component of white mineral trioxide aggregate with a phosphate-containing fluid.J Endod. 33: 1347-1351. Ref.: https://www.ncbi.nlm.nih.gov/pubmed/17963961
21. Han L, Okiji T, Okawa S. 2010. Morphological and chemical analysis of different procipitates on mineral trioxide aggregate immersed in different fluids.Dent Mater J. 29: 512-517. Ref.: https://www.ncbi.nlm.nih.gov/pubmed/20823620
22. Gandolfi MG, Taddei P, Tiniti A, et al. 2010. Apatite forming ability (bioactivity) of Pro Root MTA. Int Endod J. 43: 917-929. Ref.: https://bit.ly/2J3IKXx
23. Reyes-Carmona JF, Felippe MS, Felippe WT. 2009. Biomineralization ability and interaction of mineral trioxide aggregate and white Portland cement with dentin in a phosphate-containing fluid. J Endod. 35: 731-736. Ref.: https://www.ncbi.nlm.nih.gov/pubmed/19410094
24. Okiji T, Yoshiba K. 2009. Reparative dentinogenesis induced by mineral trioxide aggregate: a review from the biological and physicochemical points of view. Int J Dent. Ref.: https://www.ncbi.nlm.nih.gov/pubmed/20339574
25. Lee YL, Lee BS, Lin FH, et al. 2004. Effects of physiological environments on the hydration behavior of mineral trioxide aggregate. Biomaterials.25: 787-793. Ref.: https://www.ncbi.nlm.nih.gov/pubmed/14609667
26. Camilleri J. 2007. Hydration mechanisms of mineral trioxide aggregate. IntEndod J. 40: 462-470. Ref.: https://www.ncbi.nlm.nih.gov/pubmed/17459120
27. Camilleri J. 2008. Characterization of hydration products of mineral trioxide aggregate. Int Endod J. 41: 408-417. Ref.: https://www.ncbi.nlm.nih.gov/pubmed/18298574
28. Darvell BW, Wu RC. 2011. “MTA” a Hydroaulic Silicate Cement: review update and setting reaction?Dent Mater. 27: 07-22. Ref.: https://www.ncbi.nlm.nih.gov/pubmed/21353694


















