
-
Mail us:
editor@raftpubs.org
Indexing & Abstracting
Full Text
Research ArticleDOI Number : 10.36811/jphsm.2020.110014Article Views : 3Article Downloads : 3
Your Next Move: Improving the health of middle-aged men who are overweight or obese
Emma J Hennessey, Benjamin R Prance, Alya Jaffer, and Angela M. Kolen*
Department of Human Kinetics, St. Francis Xavier University, Canada
*Corresponding Author: Angela M. Kolen, Department of Human Kinetics, St. Francis Xavier University, Canada, Email: akolen@stfx.ca
Article Information
Aritcle Type: Research Article
Citation: Emma J Hennessey, Benjamin R Prance, Alya Jaffer, et al. 2020. Your Next Move: Improving the health of middle-aged men who are overweight or obes. J Phy Hea Spt Med. 3: 04-13.
Copyright: This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Copyright © 2020; Emma J Hennessey
Publication history:
Received date: 16 April, 2020Accepted date: 23 April, 2020
Published date: 24 April, 2020
Background: Your NeXt Move: X Fans in Training Program is a healthy lifestyle program tailored for men who are overweight or obese and was based on another intervention implemented in an urban setting. The goal of ‘Your NeXt Move’ was to improve men’s health through exercise and health literacy-based lessons using humor and competition to facilitate positive lifestyle changes. This paper shares the efficacy of the 12-week program regarding weight, body mass index, waist circumference, blood pressure and physical activity in 35 to 65-year-old men who were overweight and obese living in a rural area.
Methods: 25 men (49.4±8.3 yrs) provided data for this study.
Results: Upon program completion, these men experienced, on average, a significant decrease in body weight (2.1 kg, p = 0.006), BMI (0.7 kg/m2, p=0.006), waist circumference, (3.6 cm, p=0.007), and systolic (7.7 mmHg, p=0.007) and diastolic (4.3 mmHg, p=0.036) blood pressure. They also, on average, increased their daily steps by about 2000, indicating improved levels of physical activity.
Conclusion: These findings suggest ‘Your neXt Move’ was successful in improving the physiological health of the men who participated.
Keywords: Physical activity; Exercise; waist circumference; Blood pressure; Comradery
Introduction
In 2014, 62% of Canadian men were considered overweight or obese [1]. The proportion of Nova Scotians classified as obese is 27.8% higher than the national average [1]. Further, 37.5% of Nova Scotia residents are considered overweight [2]. The obesity epidemic and the underlying mechanism of weight gain stems from individuals consuming an improper intake of nutritional goods, low levels of physical activity, and living a sedentary lifestyle [3]. Hypertension is common among individuals who are obese. Neter et al [4]. found that a weight loss of 5.1 kg, or an increase in physical activity, or both led to a significant reduction in systolic (4.44 mmHg) and diastolic blood pressure (3.57 mmHg). During extended periods of sedentary behaviour, (i.e. sitting and lying with an energy expenditure of <1.5 METs) [5], large muscle groups of the trunk, legs, and back lack stimulation and therefore remain largely inactive, resulting in lower caloric expenditure that often tips energy balance in favour of weight gain [6]. Although increases in technology may result in greater sedentary behaviours [61], technology may also be used to increase physical activity. Pedometers, for example, have been shown to be useful in increasing physical activity possibly because serve as a reminder of day-to-day goals [7]. Only 17% of men in Canada meet the recommended 150 minutes of moderate or more intense physical activity per week [8]. Men are described as more reluctant to respond to health promotion or to seek medical-related assistance, health education sessions, and annual health checks [9]. The cultural construct of masculinity is partly to blame, as some men may perceive diet and exercise classes as “feminine” and are thus hesitant to participate in lifestyle interventions intended to improve their health, including weight reduction. The social construct of an idealistic masculine body is muscular and large, which allows men to feel content with being larger – even if they are obese [10]. To combat this reluctance to embrace much-needed lifestyle interventions, it has been suggested that programs aimed to improve men’s health include humour, competition, and attract like-minded individuals [11,12]. As many as 70% of men’s risk for comorbidities associated with obesity could be prevented through a healthy diet, regular physical activity, less sedentary time, smoking cessation, and reducing excess alcohol consumption [13]. A caloric expenditure of approximately 1500-2000 kcal/week via physical activity is associated with improved weight maintenance [14]. Furthermore, focusing on risk reduction and chronic disease prevention through active living and healthy eating, while utilizing effective modes of delivery and behavioural therapy in group exercise settings, has resulted in weight loss for men [9]. Previous programs, targeting men who are sports fans, have proven to be beneficial in recruitment and adherence to healthier lifestyle programs [9]. The Varsity Fans in Training (VFIT) program met these expectations in providing middle-aged men who were sport fans an environment where they could intrinsically enjoy the experience of exercising and learning in a gender-sensitized exercise and healthy lifestyle program [12,15]. In this program, 80 men lost on average 3.58 kg and sustained the weight loss for 12 months, increased their physical activity, and improved their blood pressure, diet, and perception of their health. The current study aimed to replicate these results in a rural setting. As such, the purpose of this study was to determine whether the Your NeXt Move, a 12-week educational and exercise intervention based on the VFIT program, would improve the health of men classified as overweight or obese living in a rural setting (population less than 20,000).
Methods
Research ethics approval for this study was obtained from the relevant Research Ethics Boards (ROMEO #23688) and informed consent was obtained from the men prior to data collection. Men were recruited via Twitter, an unsolicited radio interview, and word of mouth. To be eligible for the program, the men had to be between 35 and 65 years old, have a BMI ≥ 28 kg/m,2 and be okayed to participate in physical (i.e., responses on the Physical Activity Readiness Questionnaire Plus or permission from their health care provider). Eligible men provided baseline measures one week prior to program initiation. Baseline and post-program measurements consisted of height, weight, waist circumference, blood pressure, and physical activity. With shoes removed and pockets emptied, height was measured and recorded to the nearest 0.1 cm utilizing a SECA stadiometer (Hamburg, Germany). Weight was measured to the nearest 0.1 kg using a Taylor digital scale (Oak Brook, Illinois, USA). Waist circumference was measured to the nearest mm with a flexible tape measure using the Canadian Society for Exercise Physiology (CSEP, 2018) protocol. Using an appropriate-sized cuff and following several minutes of sitting quietly, blood pressure was measured using the OMRON Digital BP Monitor HEM-907. Following these measurements, participants were given pedometers (Piezo RX Steps Count) to wear for the following week, and instructed to record their daily steps for seven consecutive days. The educational and exercise program Your NeXt Move consisted of 12, 90-minute sessions held once a week. As the sessions progressed, the time allocated to the classroom component decreased with more time allocated to the exercise component as shown in Table 1. While maintaining the core, integrity, and main lessons of the original program, session content diverged slightly from the original program to meet the men’s needs and interests of this study. More specifically, topics were added based on the men’s interest and the research team’s collective expertise. Further, exercises were modified based upon limitations, fitness levels, or preferences of the group while maintaining the specificity (e.g., strength) and intensity of the exercises.
|
Table 1: Your NeXt Move Classroom Sessions and Exercise Time. |
||
|
Week |
Classroom |
Exercise |
|
1 |
Introduction to the program – including what to expect Learning about personal control regrading food and physical activity. Goal-setting |
15 minute walk |
|
2 |
Review goals, talk about how the week went; Learn about health eating SMART Goals |
25 minute walk |
|
3 |
Review goals, talk about how the week went; Learn about various types of thinking that contradict healthier behaviours Planning for healthier eating Learn about the principles of fitness |
30 minute walk Flexibility exercises |
|
4 |
Review goals, talk about how the week went; Learning about adding more physical activity daily Physical activity vs. exercise Learning about heart rate and intensity of exercises |
25 minute Aerobic exercises |
|
5 |
Review goals, talk about how the week went; Learn more about alcohol |
40 minutes Aerobic exercises |
|
6 |
Review goals, talk about how the week went; Talk about behaviour change theories Share experiences to date – manage behaviours, enhance supports |
45 minutes Strength and muscular endurance |
|
7 |
Review goals, talk about how the week went; Learn about various motivational strategies Adjust targets/goals as needed |
45 minutes Strength, muscular endurance, aerobic exercises |
|
8 |
Review goals, talk about how the week went; Learn about food labels Share more ideas for healthier eating |
45 minutes Strength, muscular endurance, aerobic exercises, flexibility |
|
9 |
Review goals, talk about how the week went; Learn about the realities of eating out – including fast foods |
45 minutes Strength, muscular endurance, aerobic exercises, flexibility |
|
10 |
Review goals, talk about how the week went; Learn about eating triggers and how to manage them Learn about sedentary behaviour triggers and how to limit them |
45 minutes Strength, muscular endurance, aerobic exercises, flexibility |
|
11 |
Review goals, talk about how the week went; Planning our eating – focusing on variety, balance, and moderation Planning our physical activity and exercise – working with setbacks |
45 minutes Strength, muscular endurance, aerobic exercises, flexibility |
|
12 |
Review goals, talk about how the week went; Celebrate completion of the program Prepare for what is next – exercising without the group |
45 minutes Strength, muscular endurance, aerobic exercises, flexibility |
For the classroom sessions, the men sat in small groups (i.e., 4-6) around round tables. The men were given a handbook at the initial session that outlined each lesson, allowed for individual goal setting, and included reference materials. The men weighed themselves weekly in a secluded area of the classroom and recorded this weight along with their participant ID on a slip of paper and placed it into a closed box. These weekly weigh-ins were for personal tracking and goal setting and not for data analysis. Table 1 shows the specific topics covered in the classroom sessions. Each session began with a review of the previous week’s goals, and the men were given time to reflect and talk about their challenges and supports in meeting these goals. The importance of ensuring SMART (i.e., specific, measureable, achievable, realistic, and timely) goals was emphasized and the men were reminded of their locus of control in relation to their eating and physical activity. In each session, the men were encouraged to set goals and include what they would do to achieve these goals directly in their handbook. The physical activity prescription involved a new goal each week, with the ultimate endpoint of increasing daily steps from baseline measure by 4500 steps per day for at least five days of the week. The men were encouraged to adjust their target if they found it too easy or difficult. The healthy eating prescription was individualized with the men choosing the parameter of healthier eating to focus on, i.e., eat one piece of fruit with each meal, drink at least eight glasses of water per day, eat three servings of vegetables, etc. The exercise prescription was for identifying a specified number of minutes of moderate to vigorous exercise to be attained outside of the program each week. Following the classroom sessions, the men took part in an exercise session as described in Table 1. Modifications to either increase or decrease the difficulty or intensity of each exercise were shared with the men to ensure their safe participation and to allow them to choose their desired workload. The exercise sessions also progressively increased in intensity using high-intensity interval training where various exercises were done for 30 seconds followed by a 30-second walk, until three sets of 30 seconds were completed for each exercise. Exercises included planks, lunges, squats, skipping, etc. These exercise sessions were designed to address the health-related components of physical fitness. Pre and post program data were analyzed using SPSS 25.0 and within subject repeated measures t-tests, to assess if there were significant changes in weight, waist circumference, BMI, blood pressure and steps. The alpha level was set at 0.05.
Results
Of the 37 men who responded to the recruitment efforts, 29 provided baseline measurements. One man was unable to start the program and three did not meet the inclusion criteria leaving 25 men (49.4±8.3 yrs) who provided baseline data and participated in the intervention program. Only 18 (72%) men provided post-program data. These men were predominantly Caucasian (96.0%), married (92.0%), and held a Bachelor’s degree or greater (68.0%). The research team encouraged attendance providing weekly emails and in-person reminders. Still, attendance was variable as shown in Table 2, with only one individual attending all 12 sessions. Absences were due to illness, work or family commitments, inclement weather, and unforeseen circumstances. Sessions were not ‘made up’ for participants who missed - although follow up email messages highlighted key topics of discussion of the sessions, including reminders of eating, physical activity, and exercise goals.
|
Table 2: Participant (n= 25) attendance for the 12-week program. |
|
|
Range of Sessions |
Number of Men |
|
≥ 10 |
6 |
|
7-9 |
9 |
|
4-6 |
6 |
|
≤ 3 |
4 |
Data Analysis
As previously noted, 18 participants provided baseline and post-intervention data. One of these men was not able to provide post-program blood pressure due to a recent surgery and only 12 men provided post-program pedometer data. Table 3 presents the men’s average height, weight, BMI, waist circumference, BP, and daily step count at baseline and post-intervention.
|
Table 3: Average (±SD) height, weight, BMI, waist circumference, blood pressure (BP), and daily steps at baseline and post-intervention for the men who took part in the 12-week program. |
||||
|
Measure |
Pre-Intervention (n= 25) |
Post-Intervention |
N (post-intervention) |
P-Value |
|
Height (cm) |
175.5±7.1 |
* |
* |
* |
|
Weight (kg) |
103.2±18.3 |
101.1±17.4 |
18 |
0.006 |
|
BMI (kg/m2) |
33.6±6.3 |
32.9±6.0 |
18 |
0.006 |
|
Waist circumference (cm) |
112.5±12.1 |
109.0±12.0 |
18 |
0.007 |
|
Systolic BP |
144.2±14.6 |
136.5±12.9 |
17 |
0.007 |
|
Diastolic BP |
87.7±6.9 |
83.4±6.9 |
17 |
0.036 |
|
7-day average of steps |
7284±3649 |
9266±4889 |
12 |
0.096 |
|
* Post-intervention height not measured. |
||||
On average, the men’s weight status improved with significant loss of weight (~2.1 kg), abdominal body fat (i.e., 3.6 cm loss in waist circumference), and lower BMI (~0.7). Further, systolic and diastolic blood pressure significantly decreased on average by 7.7 and 4.3 mm Hg, respectively. Although the men walked more on average as noted by an increase in steps of almost 2000 steps from baseline, this increase was not significant. Further evaluation of the steps data with one outlier value removed (≥ 1 SD below the mean - see participant 11 in Figure 1), showed a significant (p=0.021) increase in average steps per day between baseline (6836.8±3464.3) and post-intervention (9458.6±5079.9) for the remaining 11 participants.
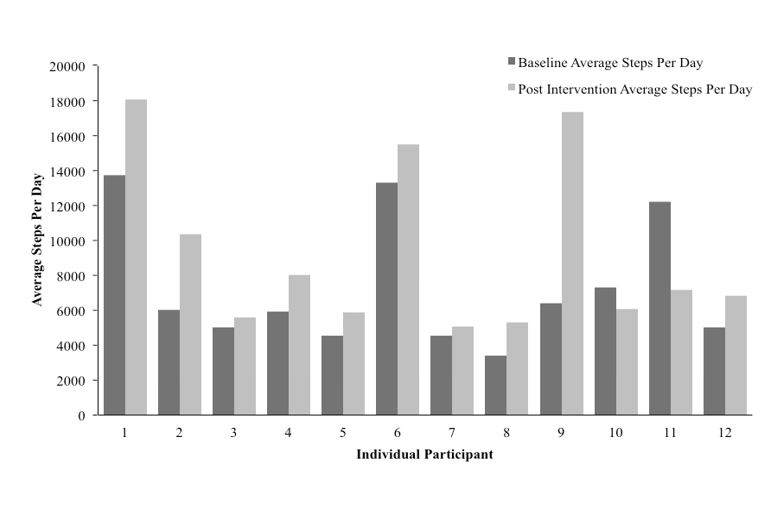
Figure 1: Baseline and post intervention average steps per day for 12 men who completed the Your Next Move intervention.
Discussion
The purpose of this study was to determine whether Your NeXt Move, a healthy lifestyle program improved the health of middle-aged men who were overweight or obese and living in a rural community. The results from this study suggest Your NeXt Move was successful as noted by a significant decrease in the participants’ average weight, waist circumference, BMI, and blood pressure, and an increase in average daily steps. The average weight loss of the group was 2.1 ± 1.8 kg. with the greatest weight loss of 6.9 kg, achieved by two participants. Petrella et al [12]. noted 30% of the men in the VFIT program achieved a weight loss of 5% or more. A 5% weight loss for our group was 5.2 kg, with 11% or 2 participants achieving this loss. The average decrease in BMI of the group was 0.67 ± 0.91 kg/m2, compared to the decrease of 1.39 ± 0.18 kg/m2 found by Petrella et al [12]. The average waist circumference decrease of the men in this study was 3.6 ± 4.9 cm, comparable to the decrease of 3.96 ± 0.81 cm found by Petrella et al [12]. Waist circumference may be a better indicator than BMI of the relationship between abdominal adiposity and risk of type 2 diabetes and other comorbidities [16,17]. As such, health benefits may occur with weight loss and in particular with loss of abdominal adipose tissue [17]. Collectively, the significant decreases in weight, waist circumference, and BMI found in the men in this study indicate an increase in health and improved prevention of the comorbidities associated with obesity. Baseline measurements of blood pressure in this study indicated the men, on average, were hypertensive (i.e. systolic BP ≥ 140 mmHg) [18]. Given the significant decrease in post-intervention blood pressure in the men, their systolic blood pressure categorization improved to normal-high. Similarly, the men’s diastolic blood pressure improved in ranking from normal-high (i.e. > 85 mmHg) to normal BP (< 85 mmHg) post-program These changes were similar to those observed in a previous VFIT program [12]. Lifestyle plays a major role in the prevalence of hypertension worldwide with excessive caloric intake and obesity identified as major causes [19]. In Your NeXt Move, the men were taught about calorie dense foods, how to monitor their eating habits, and how to make changes where necessary. The decrease in blood pressure in this study might also be attributed to the exercise component of the intervention. Exercise is commonly recommended for the prevention and treatment of hypertension [20] with decreases of 5-7 mm Hg expected following endurance exercise [21].
Although less than found by Petrella et al [12], the men took almost 2000 more steps per day or an average increase of 27.2% from baseline. This discrepancy might relate to location, in that men living in rural communities are generally less physically active overall [22]. A closer look of the data shows that 10/12 men had an average increase of (3007±3079) steps per day - closer to the goal of increasing baseline steps by 4500. The increased number of steps were a result of the men parking further away, taking the stairs more frequently, or using bathrooms located further away or on a separate floor while at work. These suggestions were shared during the classroom sessions. Similar to Gill et al [7], some men in this study were motivated by the pedometers they were given. Although attendance varied, a core group was present each week. It is believed the men were honest about their health behaviours, attentive, and focused, and discussions were in-depth regarding specific barriers faced and improvements needed. Most men were married, and this potentially influenced the success of the program. Several men mentioned their partners’ influence on their healthier lifestyle attitudes and behaviours: positively and negatively. Some men shared that their partners were reluctant to help them make dietary changes (e.g. reluctant to buy different groceries or prepare healthier meals), whereas other men’s partners were supportive and made similar behaviour changes (e.g., adding more vegetables to their meals, reducing consumption of less healthy snacks). This observation is connected to the idea that it is often the men’s partners who promote healthier lifestyle behaviours [9]. The success of Your NeXt Move is partly due to the group dynamics. The research team fostered a social environment without judgement, humorous discourse, comradery, and a theme to “sweat it out” together. The positive attitudes and friendly competition within the group made classroom discussions diverse and exercise sessions effective. Discussion and mutual learning was encouraged by the researchers to foster the relationships and to improve confidence for making healthier lifestyle choices. The participants’ commitment to the program also drove its success. A population of at-risk men were involved in this study. Men are more reluctant to respond to health promotion and to seek medical-related assistance, health education sessions on illness prevention, and annual health checks [9]. Interestingly, the men themselves spread created awareness about the program within the community with many bringing friends. Many men expressed interest from partners and/or female coworkers to become involved in the program as well. The advantage of coordinating the program in a rural area was the increased communication within the community. It can be argued that the group dynamic is stronger in a rural area, where the participants became close, often attend the same events, and have mutual connections - potentially creating improved accountability. Although the program deviated from VFIT’s original goal of recruiting sports fans to achieve this comradery, the lack of sports affiliation did not decrease the strength of this group’s connection; it is believed the men in this program were beginning to view themselves as part of the solution to their families becoming healthier. In terms of sustainability, the educational sessions gave the men many tools and tips to use in their daily lives. Arguably, engaging in formal exercise outside the sessions or following program completion would be more difficult. The reality of applied research and programs is that individuals have difficulty making and maintaining changes without the help of others. However, with the tools and lessons regarding health literacy given, these men should be able to adhere to healthier lifestyles long-term – something that only can be found with a follow up study. A limitation in this study was that follow-up data were not obtained from all men. Although there was a large enough sample (i.e., 18 men) for statistical analyses, the sample was homogenous. Most men were Caucasian, married, and had more than a high-school education. The participant group consisted of those who were presumably middle-class, potentially limiting the generalizability of the findings by overlooking populations that may not have had access to affordable exercise training, sport programs, or lacked education surrounding nutrition and healthy lifestyles. A further limitation was compliance to the program with 32% of participants attending less than half (<6) of the sessions. Efforts were made throughout the program to enhance adherence, however, only one participant attended all twelve sessions. Low attendance levels may reflect real life commitments participants encountered. It is believed that the more sessions attended, the greater the likelihood of adhering to the PA prescriptions each week. However this may not be true, as one participant was only capable of attending two of 12 sessions due to work restrictions, yet had a considerable decrease in blood pressure (systolic: -26.0 mm Hg; diastolic: -13.3 mm Hg) and the largest increase in average steps per day post-intervention (+10936 average steps per day). The mechanism by which this occurred should be further investigated though it was believed that he held himself accountable to the program through weekly updates of steps taken and weight lost shared through email. Participants were reminded that the program was not a diet or exercise program per se but rather a program that encouraged choosing a healthier, physically active lifestyle, using the ideas presented to facilitate small, sustainable changes for the long term. This program was successful in decreasing weight, waist circumference, BMI, and BP, as well as improving daily physical activity in middle-aged men classified as overweight or obese. If the objective of this program was to increase healthy behaviours and adherence to exercise and physical activity, then a key is the importance of sustainability. Implementing further programming and recruiting more student-leaders following this study (in terms of the continuation of weekly exercise sessions) is important to ensure the sustainability and accountability of the men who participated, and to offer opportunities to those who were unable to previously participate. Although Your NeXt Move was successful with once a week sessions, this program could be extended to multiple sessions per week. This would encourage adherence providing alternative dates, as well as create more formal exercise sessions per week. With this alteration to programming, it would become less debilitating for a participant to miss one session. While likely to increase attendance rates, this would require more time, resources, facility bookings, and personnel. A 12-month follow up data collection similar to previous VFIT programs could be beneficial in providing more extensive long-term results of this program. Interviewing participants and performing a qualitative analysis on the results could also be beneficial in future studies, providing an understanding of motivation, attitude, and knowledge in regards to healthy eating and PA. Understanding why some participants were able to increase their average steps per day by more than 10000 steps or investigating the reasoning for large decreases in average steps per day can be seen as valuable in assisting poisitive changes to the future of men’s health.
Acknowledgements
The authors thank the men who participated in Your NeXt Move for their comradery and passion to be part of this program.
Funding
This work was supported by the Department of Human Kinetics and the Research Grants Office at StFX.
References
1. Statistics Canada. 2015. Overweight and obese adults (self-reported), 2014. Health Fact Sheets Report 82-625.
2. Twells LK, Gregory DM, Reddigan J. et al. 2014. Current and predicted prevalence of obesity in Canada: a trend analysis. Can Med Ass J. 2: 18-26. Ref.: https://bit.ly/2VT0hrk
3. Agrawal P, Gupta K, Mishra V, et al. 2017. Effects of sedentary lifestyle and dietary habits on body mass index change among adult women in India: Findings from a follow-up study. Ecology Food Nutr. 52: 387-406. Ref.: https://bit.ly/3cK4AvV
4. Neter EJ, Stam EB, Kok JF, et al. 2003. Influence of weight reduction on blood pressure: A meta-analysis of randomized controlled trials. Hypertension. 42: 878-884. Ref.: https://bit.ly/2S2aHUu
5. Herman KM, Saunders TJ. 2016. Sedentary behaviours among adults across Canada. Can Publ Health Ass. 107: 438-446. Ref.: https://bit.ly/3eFOIN7
6. Sisson SB, Camhi SM, Church TS, et al. 2009. Leisure Time Sedentary Behavior, Occupational/Domestic Physical Activity, and Metabolic Syndrome in U.S. Men and Women. Metabol Syndr Relat Disord. 7: 529-536. Ref.: https://bit.ly/2wZZYmg
7. Gill DP, Blunt W, Cruz AD, et al. 2016. Hockey Fans in Training (Hockey FIT) pilot study protocol: A gender-sensitized weight loss and healthy lifestyle program for overweight and obese male hockey fans. BMC Publ Health. 16. Ref.: https://bit.ly/2VV0xpQ
8. Colley RC, Garriguet D, Janssen I, et al. 2011. Physical activity of Canadian adults: accelerometer results from the 2007 to 2009 Canadian health measures survey. Statistics Canada Catalogue 82-003-X Health Reports. Ref.: https://bit.ly/3eKqwZS
9. Bottorf JL, Seaton CL, Johnson ST, et al. 2011. An updated review of interventions that include promotion of physical activity for adult men. J Sport Med. 45: 775-800. Ref.: https://bit.ly/3ePiJdt
10. Hunt K, McCann C, Gray CM, et al. 2013. You’ve got to walk before you run”: Positive evaluations of a walking program as part of a gender-sensitized, weight-management program delivered to men through professional football clubs. Health Psychol. 32: 57-65. Ref.: https://bit.ly/2zj3bhv
11. Gavarkovs AG, Burke SM, Petrella RJ. 2016. Engaging men in chronic disease prevention and management programs: A scoping review. Am J Men’s Health. 10: 145-154. Ref.: https://bit.ly/3bvDjNV
12. Petrella RJ, Dawn G, Guangyong Z, et al. 2017. Hockey fans in training a pilot pragmatic randomized controlled trial. Med Sci Sport Exer. 49: 2506-2516. Ref.: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5704649/
13. Krueger H, Andres EN, Koot JM, et al. 2014. The economic burden associated with diseases in men and the contribution of tobacco smoking, excess weight, alcohol consumption and physical inactivity to this burden. Can J Publ Health. 105: 69-78. Ref.: https://bit.ly/2yziBhm
14. Williams PT, Wood PD. 2006. The effects of changing exercise levels on weight and age-related weight gain. Int J Obes. 30: 543-551. Ref.: https://go.nature.com/2VPxQLd
15. Blunt W, Gill DP, Sibbald SL, et al. 2017. Optimization of the hockey fans in training (hockey FIT) weight loss and healthy lifestyle program for male hockey fans. BMC Publ Health. 17: 916. Ref.: https://bit.ly/3asWMgz
16. Chan JM, Rimm EB, Colditz GA, et al. 1994. Obesity, fat distribution, and weight gain as risk factors for clinical diabetes in men. Diabetes Care. 17: 961-969. Ref.: https://bit.ly/2KrVzM1
17. Jingyuan F, Hofker M, Wijmenga C. 2015. Apple or pear: size and shape matter. Cell Press. 21: 507- 508. Ref.: https://bit.ly/2XXwz7p
18. Government of Canada. Hypertension. 2015. Retrieved from https://www.canada.ca/en/public-health/services/chronic-diseases/cardiovascular-disease/hypertension.html
19. Savica V. Bellinghieri G Kopple JD. 2010. The effect of nutrition on blood pressure. Ann Rev J. 30: 365-401. Ref.: https://bit.ly/2KtK2Ma
20. Diaz MK, Shimbo D. 2013. Physical activity and the prevention of hypertension. Cur Hypertension Rep.15: 659-668. Ref.: https://bit.ly/2Vvxri7
21. Pescatello LS, Franklin BA, Fagard R, et al. 2004. Exercise and hypertension. J Am Coll Sport Med. 36: 533-553. Ref.: https://bit.ly/2VLa2Ig
22. Gavarkovs AG, Burke SM, Petrella RJ. 2015. The physical activity–related barriers and facilitators perceived by men living in rural communities. Am J Men’s Health. 11: 1130-1132. Ref.: https://bit.ly/3eMwc5t


















