
-
Mail us:
editor@raftpubs.org
Indexing & Abstracting
Full Text
Case ReportDOI Number : 10.36811/jcshd.2022.110024Article Views : 46Article Downloads : 33
Surgery of polycystic cardiac disease: A case report
Redha Lakehal*, Soumaya Bendjaballah, Rabah Daoud, Khaled Khacha, Baya Aziza and Abdelmalek Bouzid
Faculty of Medicine Constantine 03, Constantine, Algeria
*Corresponding Author: Redha Lakehal, Department of Heart Surgery, Ehs Dr Djaghri Mokhtar, Constantine, Algeria; Email: lakehal.redha@gmail.com
Article Information
Aritcle Type: Case Report
Citation: Redha Lakehal, Soumaya Bendjaballah, Rabah Daoud. 2022. Surgery of polycystic cardiac disease: A case report. J Cardiovasc Surg Heart Dis. 4: 05-08.
Copyright: This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Copyright © 2022; Redha Lakehal
Publication history:
Received date: 20 December, 2021Accepted date: 30 December, 2021
Published date: 03 January, 2022
Abstract
Introduction: Cardiac localization of hydatid disease is rare (<3%) even in endemic countries. Affection characterized by a long functional tolerance and a large clinical and paraclinical polymorphism. Serious cardiac hydatitosis because of the risk of rupture requiring urgent surgery. The diagnosis is based on serology and echocardiography. The aim of this work is to show a case with polycystic cardiac disease and to shed light on the severity of this condition.
Methods: We report the observation of a 49-year-old woman with a history of unoperated hepatic hydatid cyst presenting with cardiac polycystosis. Preoperatively: NYHA stage II dyspnea. Chest xray: CTI at 0.65. ECG: Negative T wave in D I, II, III, V4, V5, V6. Echocardiography: Multiple pericardial cysts all bypassing the heart, one of which is the largest multilobed LV peri and another compressing the LA, another compressing the RA without signs of poor tolerance. Thoracic CT: Cardiopericardial polydatidosis. Intraoperative exploration: multiple cysts, which are developed at the expense of the heart, located at the level: roof of the LA; free wall of the RV; of the IV septum LA and the LV. Gesture: puncture; aspiration of cysts; removal of daughter vesicles and sterilization of residual cavities with hypertonic saline. Results: The postoperative consequences were simple.
Conclusion: The simultaneous presence of several hydatid cysts in the heart is not uncommon, but cardiac localization is rare; serious and can constitute a real surgical emergency, hence the importance of prevention.
Keywords: Hydatid cyst of the heart; Polycystosis; Surgery; Extracorporeal Circulation; Prevention
Introduction
Cardiac localization of hydatid disease is rare (<3%) even in endemic countries [1]. Affection characterized by a long functional tolerance and a large clinical and paraclinical polymorphism [2]. Serious cardiac hydatitosis because of the risk of rupture requiring urgent surgery. The diagnosis is based on serology and echocardiography [2-3]. Computed tomography (CT) and magnetic resonance imaging (MRI) are the other diagnostic tools. The treatment of cardiac hydatid cysts is surgery [3-4]. The aim of this work is to show a case with polycystic cardiac disease and to shed light on the severity of this affection.
Case report
We report the observation of a 49-year-old woman with a history of unoperated hepatic hydatid cyst presenting with polycystic cardiac disease discovered incidentally during echocardiography due to exertional dyspnea. Functionally, the patient had dyspnea stage II of NYHA. Chest x-ray showed a cardiothoracic index at 0.65 with deformities of the heart contours. ECG was registered in regular sinus rhythm with negative T wave in D I, II, III, V4, V5, V6. Echocardiography showed multiple pericardial cysts all bypassing the heart with the largest multilobed left ventricular (LV) peri-ventricular (LV) and another compressing the left atrium (LA), another compressing the right atrium (RA) (Figure 1) without signs of poor tolerance with left ventricular dysfunction with EF: 45%.

Figure 1: Transthoracic echocardiographic image of polycystic heart disease.
Thoracic computed tomography (CT) showed cardio-pericardial polyhydatidosis with 10 cysts of different ages and sizes (Figure 2).
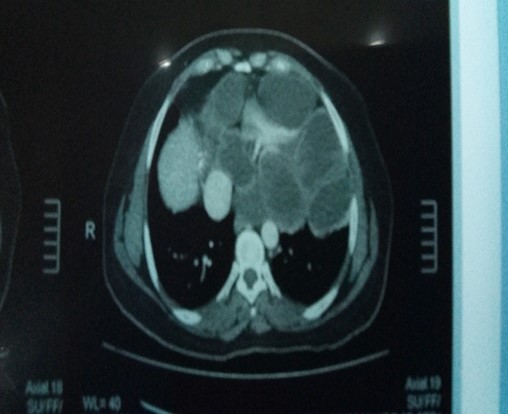
Figure 2: CT image of polycystic heart disease.
Hydatid serology was positive. The patient was operated on under cardiopulmonary bypass. The hypertonic saline serum sponges were placed into the pericardial cavity to prevent contamination. Intraoperative exploration showed multiple cysts which are developed at the expense of the heart, located at the level: roof of the left atrium (LA); free wall of the right ventricle (RV); of the interventricular septum and the left ventricle (LV). (Figure 3.4). Gesture consisted of puncture and aspiration of cysts contents; ablation of vesicles and germinal membranes, sterilization of the residual cavities with 30% hypertonic saline serum and finally padding of each residual cavity (Figure 3,4).

Figure 3: The operation view, puncture of a hydatid cyst of the RV.
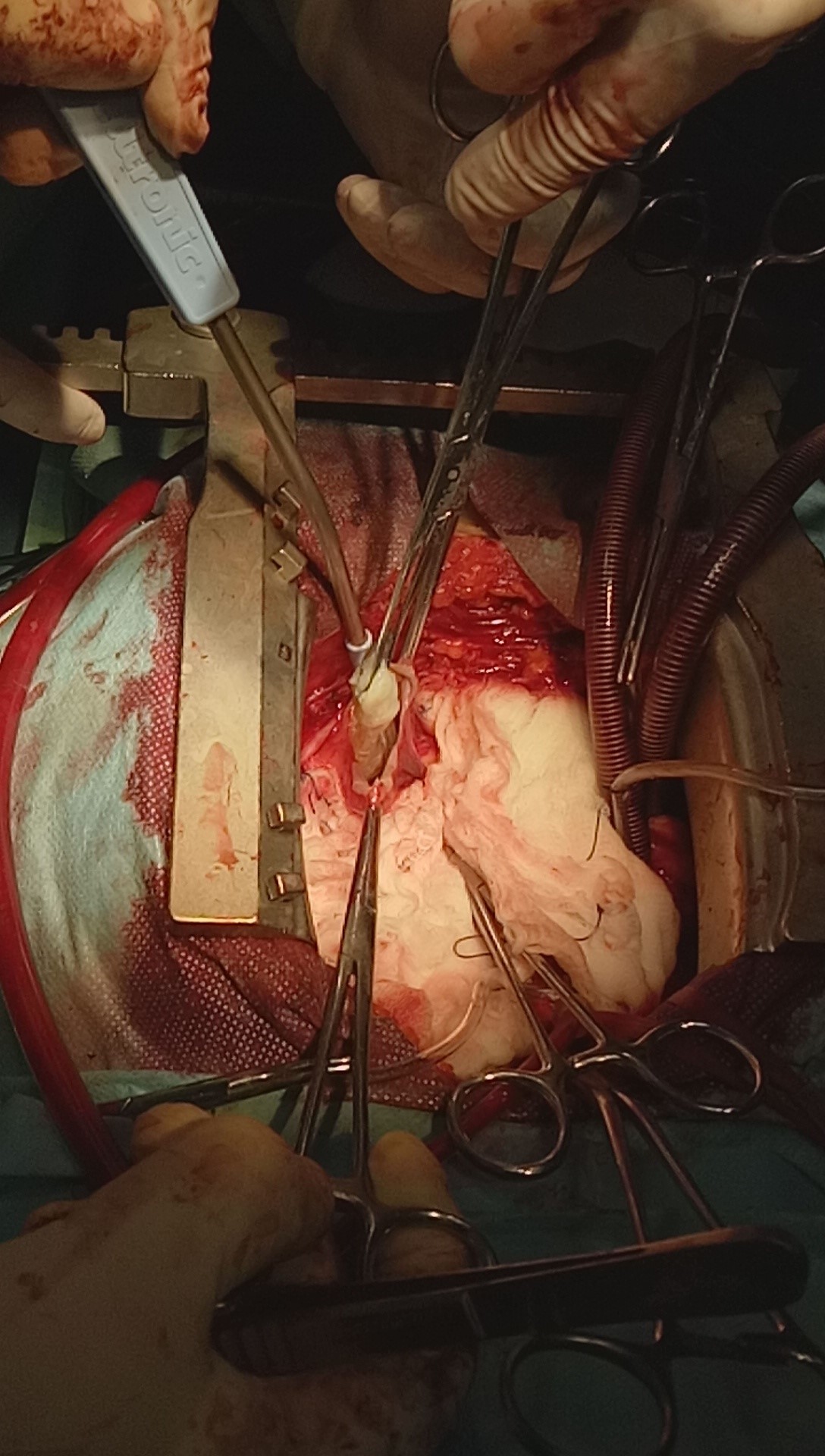
Figure 4: The operation view, evacuation of hydatid cyst contents from the RV.
After the operation, there was no problem in the intensive care unit. The patient was discharged at the first postoperative week. The patient is still on albendazole treatment at the rate of 01 tablet/ day for a year. The immediate and distant postoperative suites were favorable.
Discussion
In addition to the risk of rupture of these cardiac cysts there are other complications such as the compression of neighboring structures such as the coronary arteries as is the case with our patient who presents with repolarization disorders; dysfunction of the two ventricles linked to the development of cysts in the full myocardium, as is the case with our patient who presents with left ventricular dysfunction [5]. Putting the patient on medical treatment based on Albendazol for a year is necessary in order to avoid the recurrence of hydatid disease, especially since the patient has not yet operated there for her hepatic hydatid cyst and she is still staying in an endemic area of hydatid disease [4].
Conclusion
The simultaneous presence of several hydatid cysts in the heart is not uncommon, but it is serious. Echocardiography is the test of choice for the detection of cardiac hydatid cyst. The indication for surgery is definite in all cases of a heart cyst because the spontaneous development is fatal. The real treatment for parasitic disease is echinococcosis control based on preventive measures that aim to interrupt the life cycle within hosts, health education and legislation.
References
1. Shehatha J, Alward M, Saxena P. 2009. Surgical management of cardiac hydatidosis. Tex Heart Inst J. 36: 72-73. Ref.: https://pubmed.ncbi.nlm.nih.gov/19436793/
2. Ipek G, Omeroglu SN, Goksedef D. 2011. Large cardiac hydatid cyst in the interventricular septum. Tex Heart Inst J. 38: 719-722. Ref.: https://pubmed.ncbi.nlm.nih.gov/22199447/
3. Orhan G, Ozay B, Tartan Z. 2008. Trente-neuf ans d’expérience Surgery of cardiac hydatid cysts. An experience of 39 years. 57. Ref.: https://pubmed.ncbi.nlm.nih.gov/17568556/
4. Funda Y, Bar?? T, Adnan TK. 2014. Cardiovascular Surgery and Interventions. 1: 3-5.
5. Yaliniz H, Tokcan A, Salih OK. 2006. Surgical treatment of cardiac hydatid disease: A report of 7 cases. Tex Heart Inst J. 33: 333-339. Ref.: https://pubmed.ncbi.nlm.nih.gov/17041691/


















