
-
Mail us:
editor@raftpubs.org
Indexing & Abstracting
Full Text
Case ReportDOI Number : 10.36811/jcshd.2021.110020Article Views : 25Article Downloads : 27
Trimetazidine may normalize left ventricular systolic function and U wave polarity in severe calcific aortic stenosis
S.R. Mittal
Department of Cardiology Mittal Hospital & Research Centre, Pushkar Road, Ajmer (Raj.), India
*Corresponding Author: Dr. S.R. Mittal, D.M. (Cardiology), Department of Cardiology Mittal Hospital & Research Centre, Pushkar Road, Ajmer (Raj.) -305001, India, Email: drsrmittal@gmail.com
Article Information
Aritcle Type: Case Report
Citation: S.R. Mittal. 2021. Trimetazidine may normalize left ventricular systolic function and U wave polarity in severe calcific aortic stenosis. J Cardiovasc Surg Heart Dis. 3: 01-09.
Copyright: This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Copyright © 2021; S.R. Mittal
Publication history:
Received date: 28 December, 2020Accepted date: 08 March, 2021
Published date: 11 March, 2021
Abstract
A case of severe calcific valvular aortic stenosis with reduced left ventricular ejection fraction is presented. Patient did not agree for surgery. He was advised trimetazidine (60 mg twice a day) in addition to Torsemide, Digoxin, Aspirin and Clopidogrel. After one month, patient showed significant improvement in symptoms, normalization of U waves in electrocardiogram and significant improvement in ejection fraction. Metabolic effects of trimetazidine could be responsible for improvement in left ventricular function in spite of no change in aortic stenosis.
Keywords: Aortic valve stenosis; Electrocardiography; Left ventricular systolic function; Trimetazidine; U wave
Introduction
Trimetazidine improves myocardial function by having an effect on its metabolism. Conventionally it is advocated for the management of myocardial ischemia. We have seen a patient of critical aortic stenosis where empirical use of Trimetazidine resulted in significant improvement in left ventricular systolic function and increase in amplitude of ‘U’ wave. To the best of our knowledge, such an effect of Trimetazidine has not been reported in past.
Case Report
A 55 years male presented with effort breathlessness and orthopnoea. Electrocardiogram (figure 1) showed sinus rhythm at a rate of 99/minute, left atrial enlargement, left ventricular hypertrophy, non-progression of ‘r’ from V1 to V4, ST segment depression in leads I, aVL, V5, V6 and small ‘U’ wave in lead V3. Echocardiography revealed severe degenerative valvular stenosis with moderate aortic regurgitation. Peak and mean gradients across aortic valve were 82.9 mm Hg and 50.9 mm Hg respectively (figure 2). There was diffuse hypokinesia. Two-dimensional ejection fraction was 20% (figure 3). Antero-posterior dimension of left atrium was 4.7 cm (figure 4a). End - diastolic and end-systolic M - mode dimensions of left ventricle from left parasternal long axis view were 6.7 cm and 5.2 cm respectively (figure 5). Mitral valve E - point septal separation was 2.3 cm (Figure 6). There was mild pericardial effusion (figure 7 a and b). Patient was advised coronary angiography and aortic value replacement. He did not agree. He was advised Tab Lanoxin 0.125 mg once daily, Tab Torsemide 40 mg once daily, Tab - Aspirin 75 mg once daily, Tab- Clopidogrel 75 mg once daily, Tab- Atorvastatin 20 mg once daily and sustained release preparation of Trimetazidine 60 mg twice a day. After one month, patient showed significant improvement in symptoms. Electrocardiogram showed normal P wave and prominent positive ‘U’ wave in leads V1 to V6 (figure 8). Repeat echocardiogram showed two - dimensional left ventricular ejection fraction of 51% (figure 9), aortic valve gradients of 119 mm Hg (peak) and 70 mm Hg (mean) (figure 10), left ventricular M-mode dimensions of 5.7 cm (end diastolic) and 3.5 cm (end systolic) (figure 11) and mitral value E point - septal separation of 1.1 cm (figure 12).
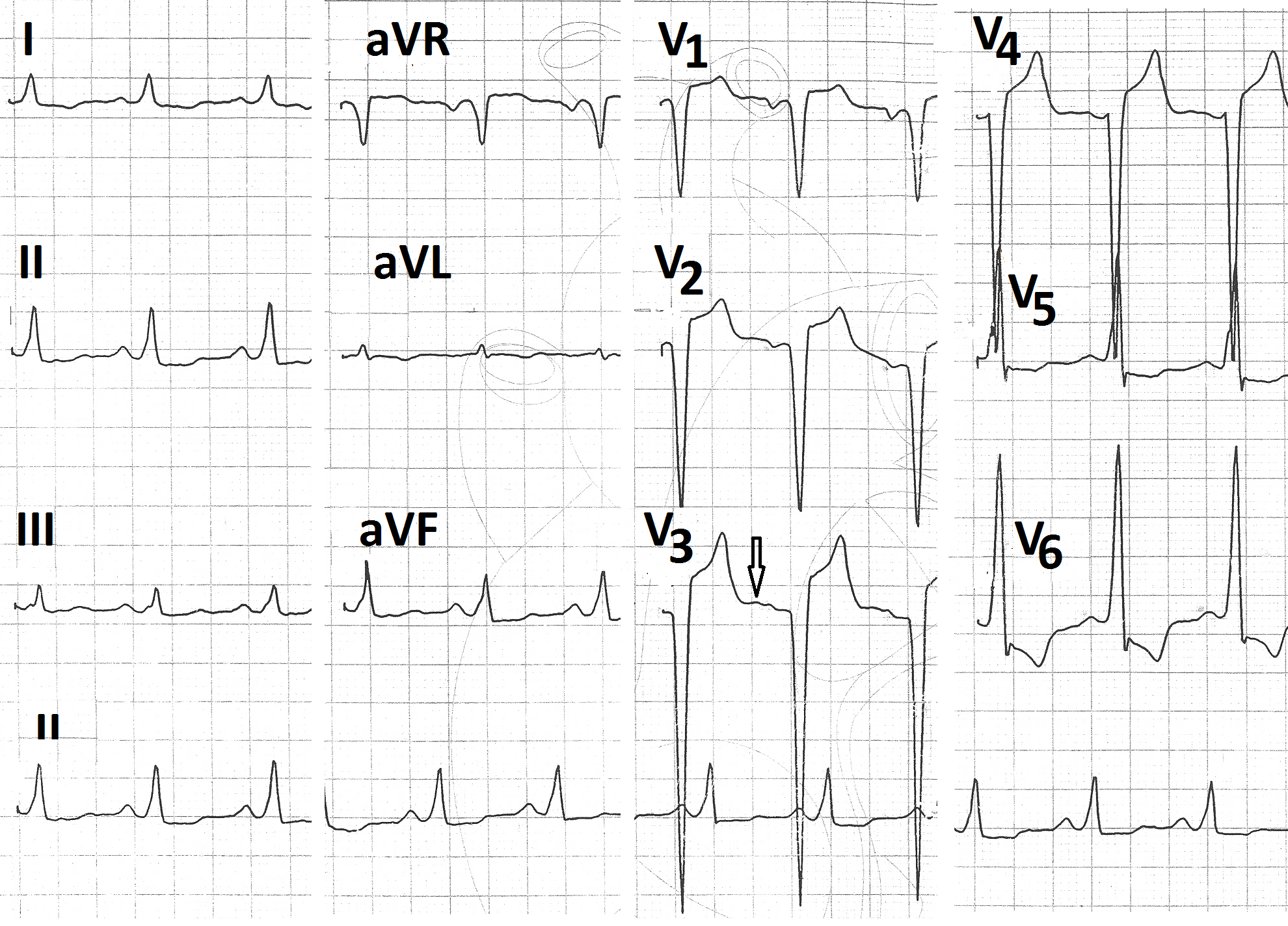
Figure 1: Pre-treatment electrocardiogram showing sinus rhythm, prominently negative P wave in lead V1, deep S wave in leads V3,V4, non-progression of ‘r’ from lead V1 to V4, ST segment depression in leads I, aVL, V5,V6 and very small U wave in lead V3 (arrow).
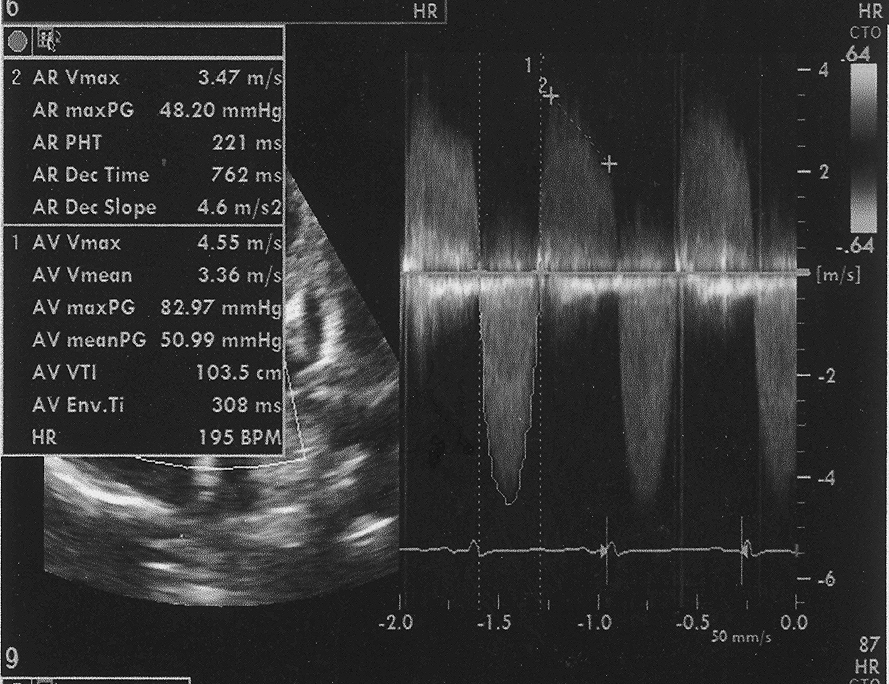
Figure 2: Doppler evaluation of aortic valve showing peak gradient of 82.9 mm Hg and mean gradient of 50.9 mm Hg with moderate AR.
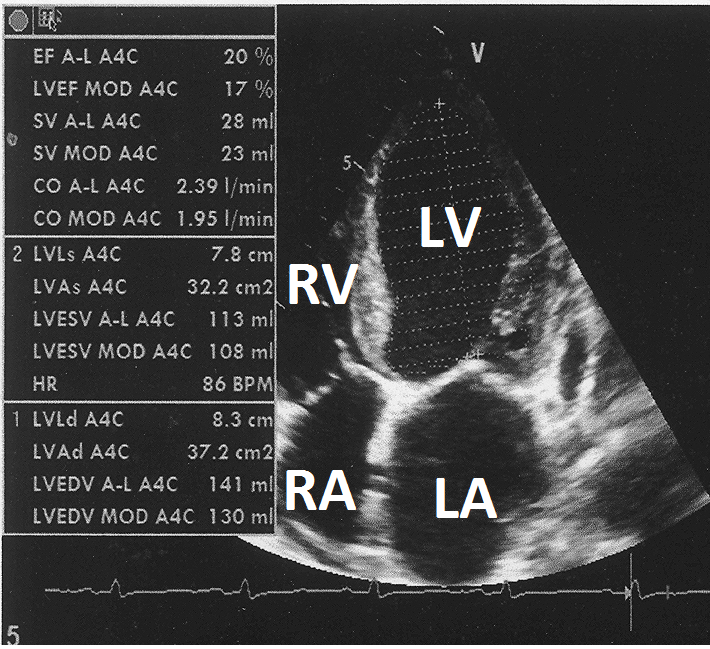
Figure 3: Two-dimensional echocardiogram from apical four chamber view showing left ventricular ejection fraction of 20% by Simpson method.
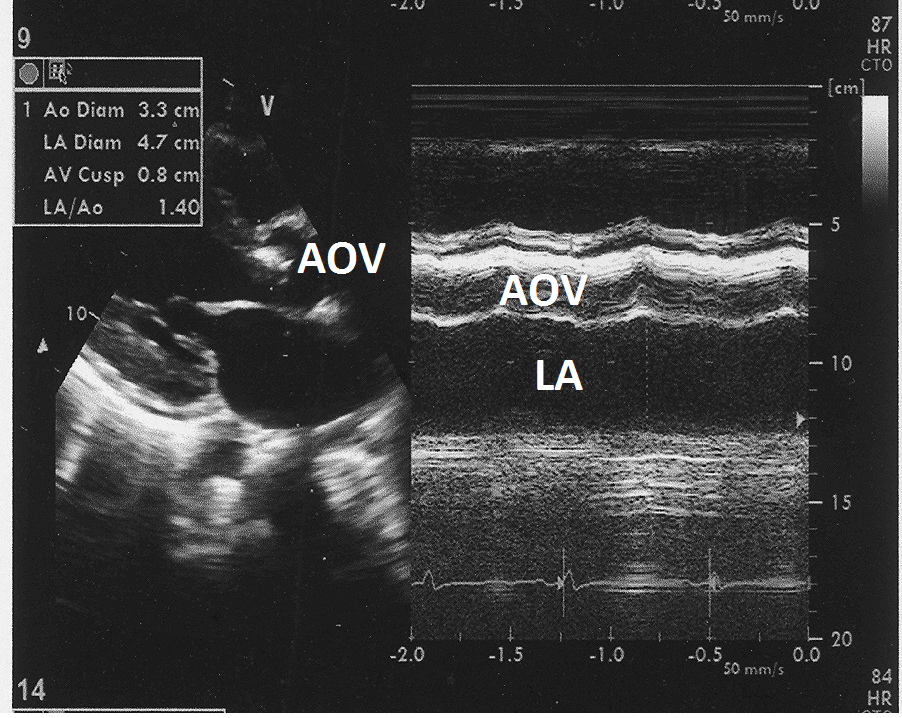
Figure 4: M mode echocardiogram from parasternal long axis view at the level of aortic root showing calcified aortic valve (AV) and left atrial dimension of 4.7cm.
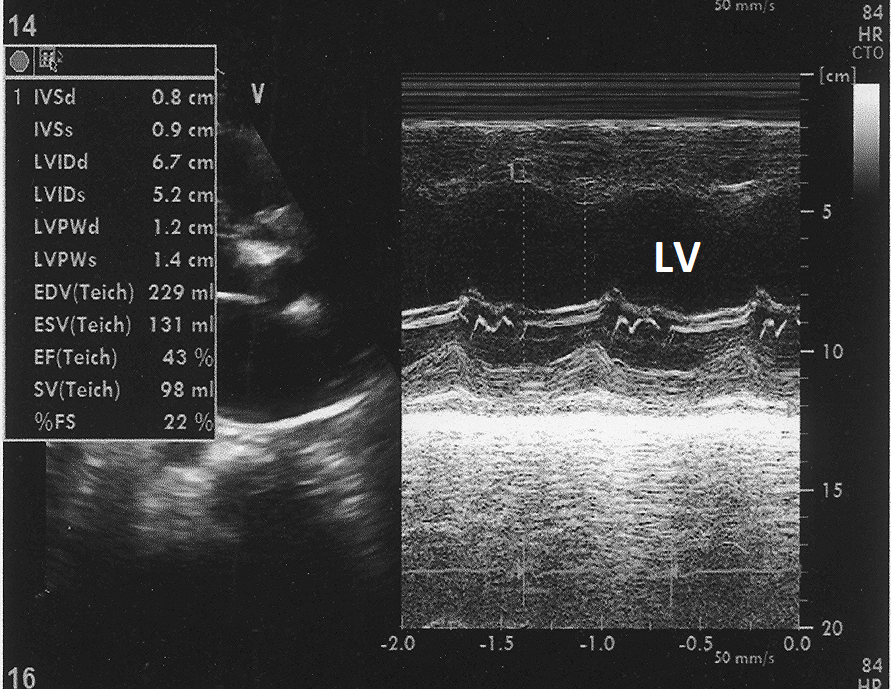
Figure 5: M- mode echocardiogram from parasternal long axis view at the level of left ventricle showing LV end diastolic dimension of 6.7 cm and end systolic dimension of 5.2 cm.
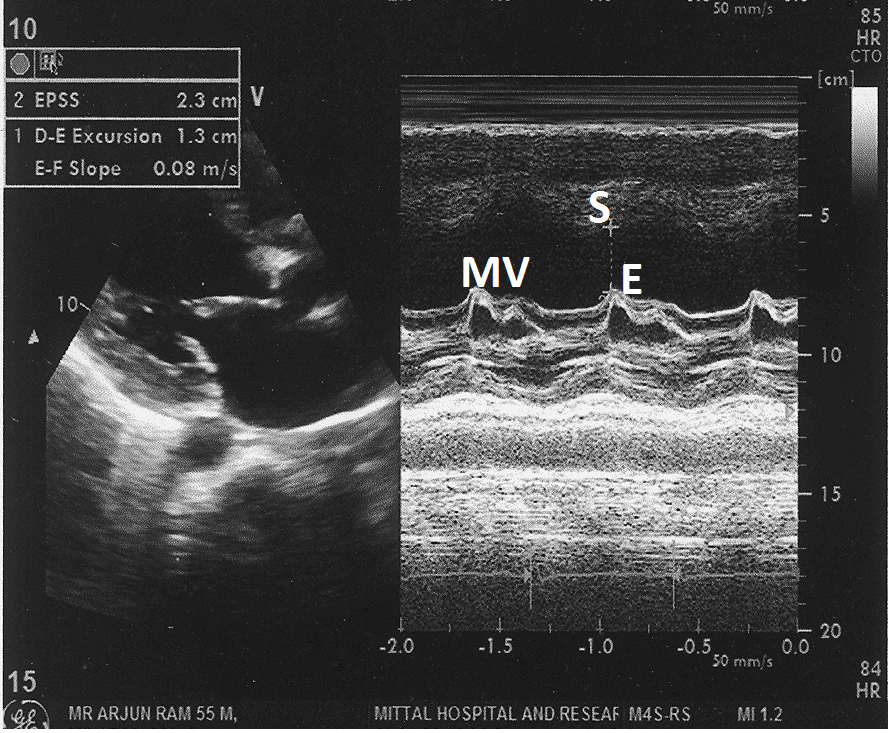
Figure 6: M- mode echocardiogram from parasternal long axis view at the tip of mitral valve showing mitral valve - E point septal separation of 2.3 cm.
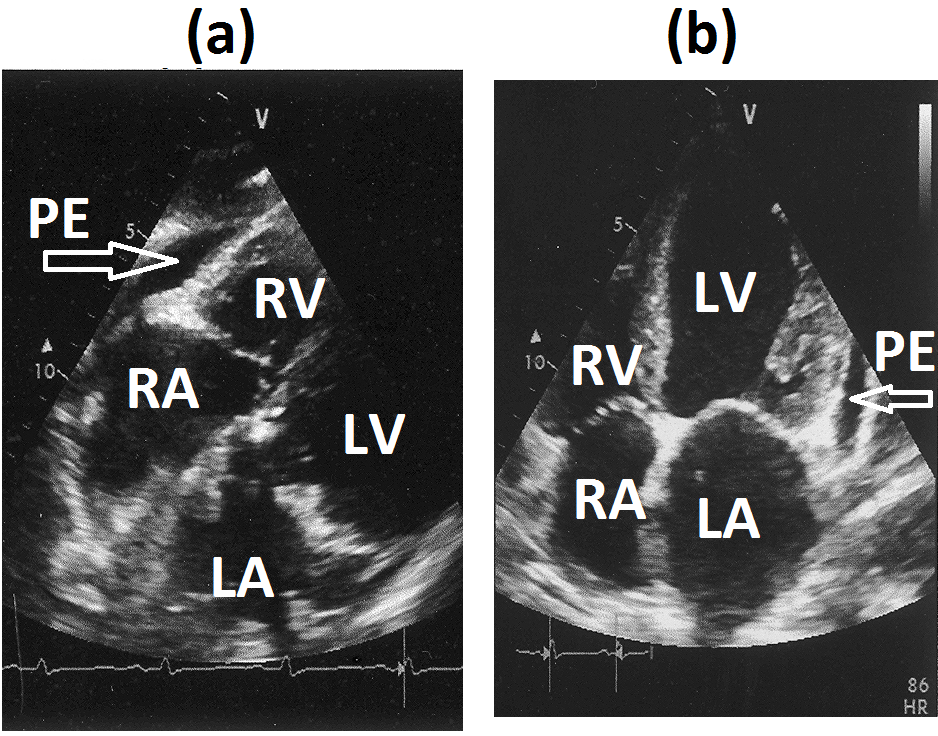
Figure 7(a): Subcostal four chamber view and (b) apical four chamber view showing minimal pericardial effusion (marked as arrow).
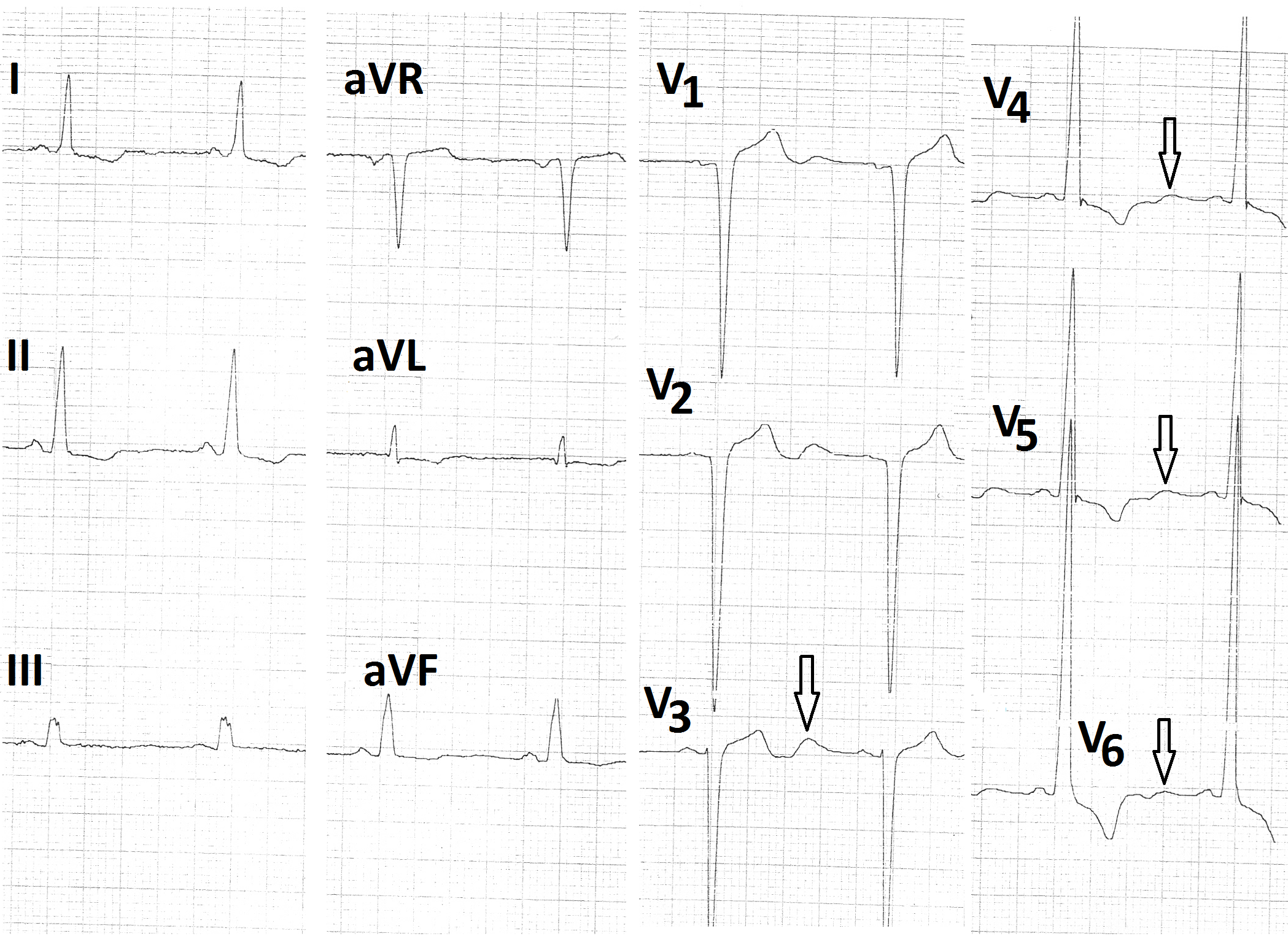
Figure 8: Post treatment electrocardiogram showing normal P wave in lead V1 and prominent positive U waves in leads V1 - V6 (arrow).
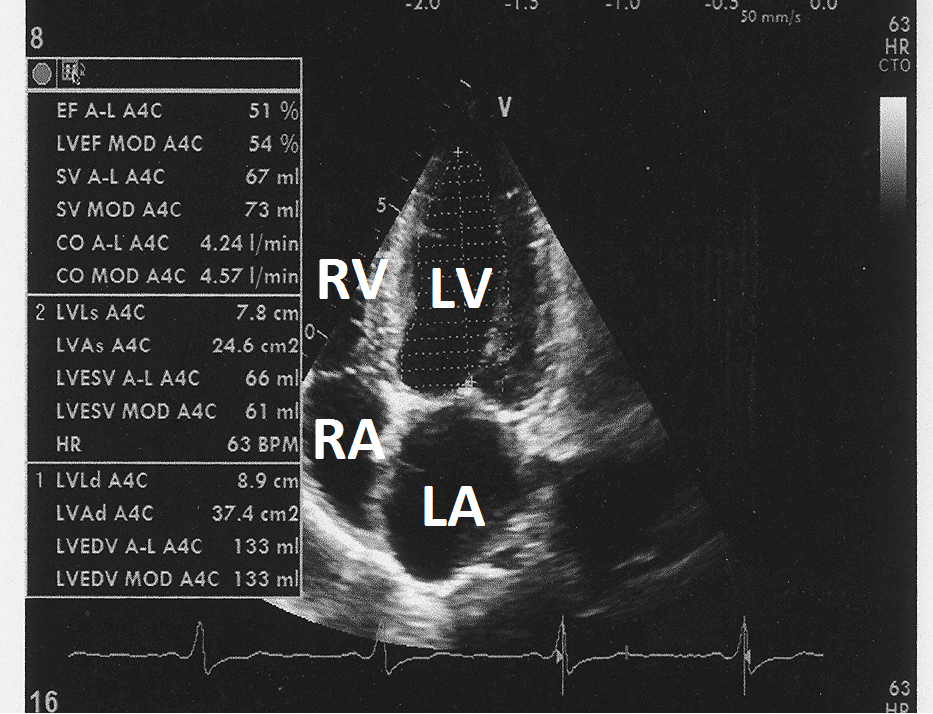
Figure 9: Post treatment two-dimensional echocardiogram in apical four chamber view showing left ventricular ejection fraction of 50% by Simpson method.
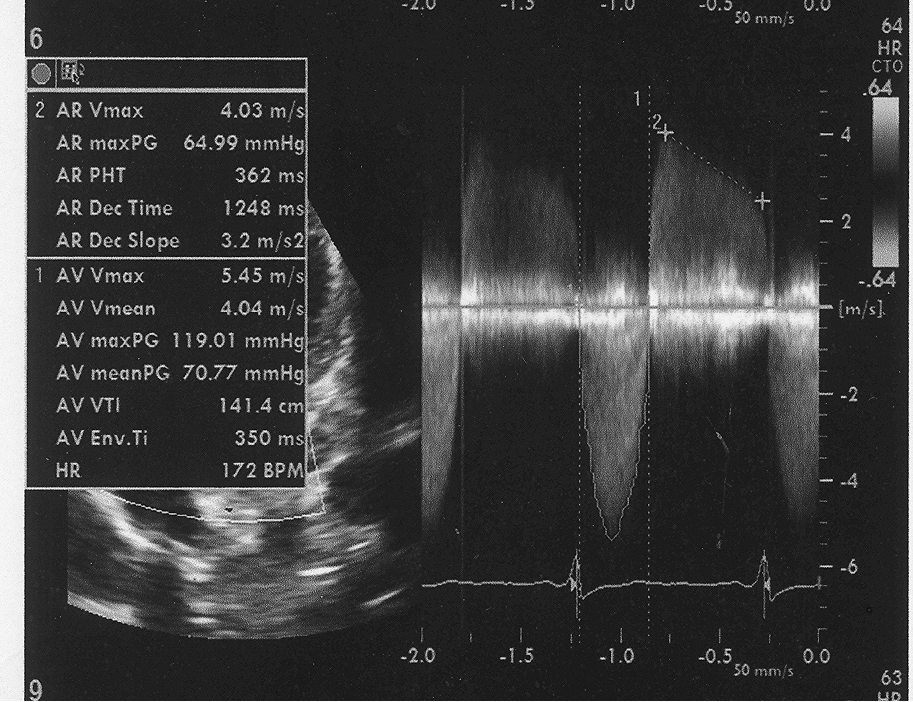
Figure 10: Post treatment peak aortic valve gradient of 119 mm Hg and mean aortic valve gradient of 70 mm Hg.
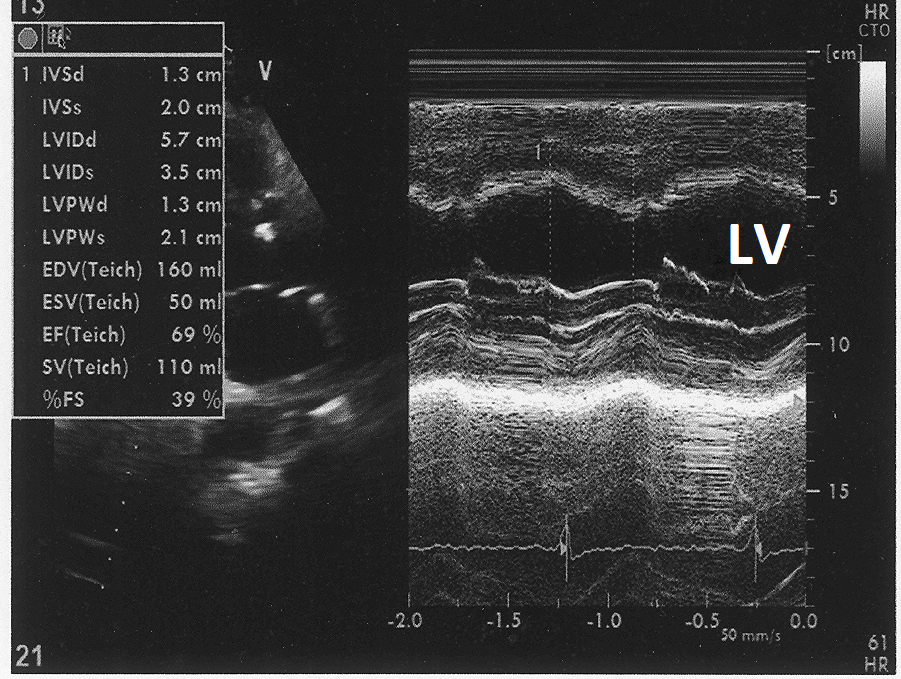
Figure 11: Post treatment M mode echocardiogram from parasternal long axis view at the level of left ventricle showing LV - end diastolic dimension 5.7cm end LV and systolic dimension of 3.5 cm.
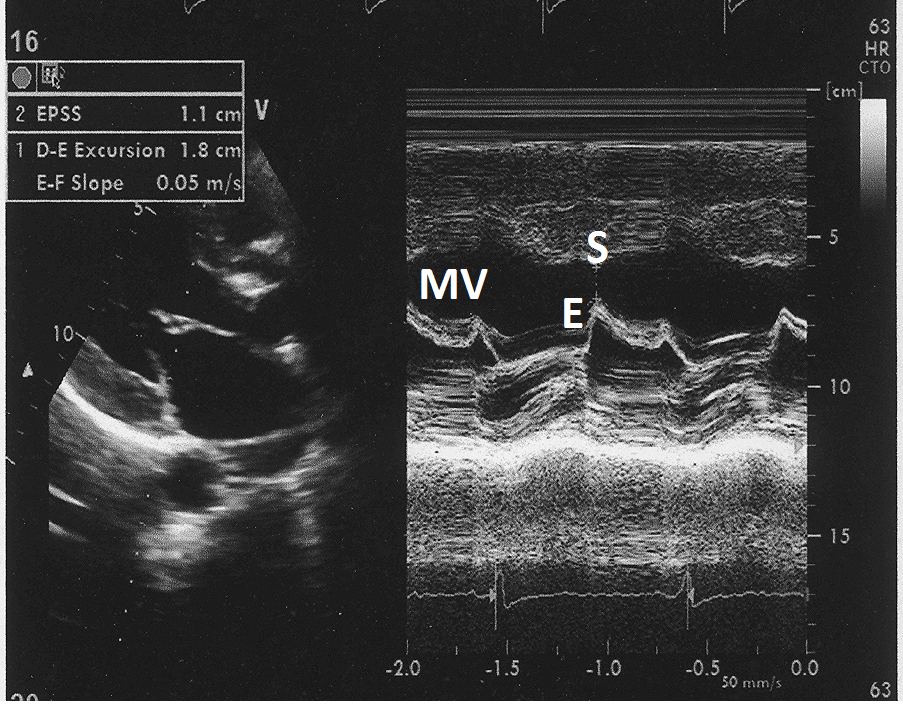
Figure 12: Post treatment M- mode echocardiogram from parasternal long axis view at the level of tip of mitral valve showing mitral valve E Point-septal separation of 1.1 cm.
Discussion
First evaluation of our patient revealed severe valvular aortic stenosis with left ventricular systolic dysfunction. Following medical treatment, there was significant improvement in left ventricular systolic function. Symptomatic relief in breathlessness could be because of diuretics. Aspirin, Clopidogrel, Atorvastatin, and low doses of Digoxin are not expected to produce significant improvement in echocardiographic variables of systolic dysfunction of left ventricle in setting of severe valvular aortic stenosis. Trimetazidine can improve myocardial function as it shifts myocardial metabolism from fatly acid to glucose use [1]. Trimetazidine has been shown to have cardiac and extracardiac benefits in idiopathic dilated cardiomyopathy [2]. It is likely that similar mechanisms were beneficial in our case of severe aortic stenosis with left ventricular systolic dysfunction. U wave of electrocardiogram follows T wave. It is usually best seen in leads V2 and V3 Its polarity is the same as that of preceding T wave and amplitude is less than 0-1 mv3. Electrophysiological basis of genesis of U wave is not clear [3]. Delayed repolarization of myocardium, late repolarization of Purkinje fibres or long action potential of mid - myocardial cells are considered as possibilities [3]. U wave amplitude increases with increasing heart rate during treadmill stress test in persons without cardiovascular disease [4]. This shows that increase in sympathetic drive could affect genesis and amplitude of U wave. Exercise induced ischemia is associated with inversion of U wave [5]. It is likely that Trimetazidine induced shift of myocardial metabolism from fatty acid to glucose could be responsible for improvement in myocardial function and increased positivity of U wave. Our case shows that increase in positivity of U wave suggests improved myocardial function. Our case shows that Trimetazidine can help patients of severe aortic stenosis with left ventricular systolic dysfunction who are not willing for surgery. Our hypothesis needs confirmation from study of myocardial metabolism. Study is also needed in patients without LV systolic dysfunction to find if Trimetazidine alone has any independent effect on amplitude of U wave. It is also possible that our case had significant coronary artery disease and the benefit observed from Trimetazidine was due to relief in myocardial ischemia. Study in patients with critical aortic stenosis with normal coronary angiograms are needed to answer if Trimetazidine could improve myocardial function in patients of critical aortic stenosis with normal coronary arteries.
References
1. Giugliano RP, Braunwald E. 2019. Non-ST elevation acute coronary syndromes. In Zipes DP, Libby P, Bonow RO, Mann DL, Tomaselli GF ed. Braunwald’s Heartdisease, Elsevier, Philadelphia. 1181-1208.
2. Tuunanen H, Engblom E, Naum A, et al. 2008. Trimetazidine, a metabolic modulator, has cardiac and extracardiac benefits in idiopathic dilated cardiomyopathy. Circulation. 48: 125-128. Ref.: https://pubmed.ncbi.nlm.nih.gov/18765391/ DOI: 10.1161/CIRCULATIONAHA.108.778019
3. Mirvis DM, Goldberger AL. Electrocardiography. et al. 2019. Braunwald’s HeartDisease, Elsevier Philadelphia. 117-151.
4. Mittal SR. 2020. U wave amplitude increases during exercise in persons without cardiovascular disease. J Cardiol Cardiovasc Res. 1: 1-9.
5. Raveendran JS, Hodfiedl R, Petkar S, et al. 2012. Significance of exercise induced U wave inversion as a marker for coronary artery disease. BMJ Case Rep. Ref.: https://pubmed.ncbi.nlm.nih.gov/22665396/ DOI: 10.1136/bcr.04.2011.4132


















