
-
Mail us:
editor@raftpubs.org
Indexing & Abstracting
Full Text
Review ArticleDOI Number : 10.36811/ijbm.2021.110024Article Views : 29Article Downloads : 28
A Tribute to Experimental Physiology
Elroy Patrick Weledji
Department of Surgery, Faculty of Health Sciences, University of Buea, Buea, SW Region, Cameroon
*Corresponding Author: Elroy Patrick Weledji, Associate Professor of Anatomy and Surgery, Department of Surgery, Faculty of Health Sciences, University of Buea, Buea, SW Region, Cameroon, Tel: 237699922144; Email: elroypat@yahoo.co.uk
Article Information
Aritcle Type: Review Article
Citation: Elroy Patrick Weledji. 2021. A Tribute to Experimental Physiology. Int J Biol Med. 3: 21-35.
Copyright: This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Copyright © 2021; Elroy Patrick Weledji
Publication history:
Received date: 08 September, 2021Accepted date: 15 September, 2021
Published date: 17 September, 2021
Abstract
Human physiology is the basis of any rational system of medicine. Experimental physiology gives insights into fundamental homeostatic and adaptive responses in health and further the knowledge of pathological mechanisms in diseases. Traditionally, a great deal of experimental physiology is done with mammalian and sub-mammalian vertebrates, frogs and toads but, increasing use is being made of experiments on human subjects, including the students themselves. The results of clinical investigations of hospital patients may also yield more detailed and relevant information than can be obtained from animal preparations. The interaction and collaboration between the scientist who aims to understand the functioning of the human body and the physician who aims to treat the malfunction is mandatory in modern medicine. This is corroborated by the fact that medicine is an art based on science.
Keywords: Experimental Physiology; History; Tribute; Biography; Medicine
Introduction
Many processes in living systems can be satisfactorily interpreted in isolation as physicochemical processes of which the mechanism is understood. However, the organization of living systems makes them more than the mere sum of their physicochemically explicable parts [1]. Many principles and processes of healthy function operate equally in disease, so that the relevance of physiology (the functioning of the human body) is not limited to the healthy. In addition, diseases are essentially disorders of physiological function and, many diseases are natural experiments which can be of great value in showing how variables and systems act upon each other. Physicians recognize and distinguish diseases by symptoms and signs which are further disorders of function revealed by close observation or elicited by testing routines. The aim of the study was to elucidate aspects of physiology in medicine through a tribute to experimental physiology from the 17th to the 20th century (Table 1).
Discussion
The publication in 1628 of William Harvey’s “An Anatomical Dissertation upon the Movement of the Blood in Animals” is usually identified as the beginning of modern experimental physiology as it demolished the ancient Galenic myths [2]. This was corroborated by the Italian biologist and physician, Marcello Malpighi’s discovery of the capillaries in 1667 [3]. However, these studies were based only on anatomical experiments. Despite increased knowledge in physics and chemistry during the 17th century, physiology remained closely tied to anatomy and medicine. Albrecht von Haller, (1708- 1777), a pupil of Herman Boerhaeve, graduated from University of Leiden (Holland) at age 21 and became a giant of the 18th century being eminent as anatomist, physiologist and botanist. In 1747 in Berne, Switzerland he published the first manual for physiology. As a professor in Bern and Gottingen he made prolific contributions to physiology, anatomy, botany, embryology, poetry and scientific bibliography. Haller’s exhaustive biological experimentation between 1757 and 1766 led to the publication of 8 volumes of the encyclopaedic Elementa Physiologiae Corporis Humani which was a landmark in medical history. Thus, the reasons for being referred to as the father of modern physiology [4]. The French aristocrat, chemist and meticulous experimenter, Antoine Lavoisier (1743-1794), along with the work of the British chemists such as Joseph Priestley was central to the 18th century chemical revolution with the origin of his discoveries about elements. His influence on the history of biology manifested at the end of the century with his writings on the physiological problems of respiration and the production of heat via combustion (metabolism) by animals [5]. After the French Academy of Science was suppressed in 1793 by the revolutionary committee, he was arrested and executed without trial in1794, and thus perished was the most illustrious victim of the revolution. Physiology as a distinct discipline utilizing chemical, physical, and anatomical methods began to develop in the 19th century. Claude Bernard in France, Johannes Muller, Justus von Liebeg, and Carl Ludwig in Germany, and Sir Michael Foster in England may be numbered as the founders of physiology as it is now known. It has been said that, if Muller provide the enthusiasm and Bernard the ideas for modern physiology, Carl Ludwig provided the methods. During his medical studies at the University of Marburg in Germany, Carl Ludwig applied new ideas and methods of the physical sciences to physiology. In 1847 he invented the kymograph, a cylindrical drum used to record muscular motion, changes in blood pressure (figure 3), and other physiological phenomena in addition to significant contributions to the physiology of circulation and urine secretion. In 1869, Ludwig founded the physiological institute in Leipzig which served as a model for research institutes in medical schools worldwide. The chemical approach to physiological problems developed in France by Lavoisier, was expanded in Germany by Justus von Liebig with books on organic chemistry and its applications to agriculture and physiology (1840) and animal chemistry (1842). The devotion to the study of physiological chemistry in the German schools evolved from Liebig’s laboratory at Giessen.
Claude Bernard (1813-1878) (figure 1) was the founder of experimental physiology in the modern sense. His experimental researches involved almost all fields of physiology, including digestive physiology of the pancreas, gluconeogenesis in the liver, the vasomotor mechanisms, the mechanisms of action of curare and the cardiac output. Francois Magendie (1783-1855), a French Physician, experimental physiologist and teacher of Claude Bernard is considered by some as the father of experimental physiology [6]. Magendie made substantial contributions to neurophysiology and in 1822 confirmed and elaborated the observation in 1811 by Charles Bell (1774-1842) the Scottish anatomist and surgeon, of the existence of both motor and sensory nerves which have separate paths to and from the spinal cord (the ventral and dorsal roots respectively) . This differentiation of spinal nerves known as the Bell-Magendie’ law is a fundamental aspect of the organization of the nervous system [7]. However, Claude Bernard’s researches established the foundation of modern physiology and biochemistry. Along with the works of Ivan Pavlov (1849-1936), the Russian physiologist and student of Carl Ludwig, on conditioned reflexes based on the associations between an environmental stimulus and another stimulus which occurs naturally, initiated physiology and psychology. His experiments on the digestive system included surgically extracting portions of the digestive system from animals, severing nerve bundles to determine the effects, and implanting fistulas between digestive organs and an external pouch to examine the organ’s contents. These earned him the 1904 Nobel prize in Physiology and Medicine [8,9]. Claude Bernard, however, is the first systems biologist as his concept of the constancy of the internal environment (le mileu interieu) implied the existence of control processes to achieve this and forms the basis of homeostasis [10] (figure 2). Claude Bernard in 1877 gave the first report on hyperglycaemia in stress from haemorhage, thus, disclosing the glycogenic function of the liver and the drastic change in biological thought of plants being the sole source of glycogen [11]. In acute haemorrhage, there is resistance of the hormone, insulin and hyperglycaemia occurs so as to achieve fluid movements and plasma refill [12]. Walter Bradford Cannon (1871-1945), an American physiologist at Harvard Medical School expanded the concept of homeostasis and coined the term ‘fight or flight response’ (the defense reaction) to a perceived harmful event through the secretion of catecholamines from the adrenal medulla which is also inhibitory to insulin [13]. This response is recognized as the first stage of the general adaptation syndrome that regulates stress responses via its mostly catabolic and cardiovascular effects among vertebrates and other organisms. Insulin resistance is a marker of surgical stress and cytokines (inflammatory peptides) hypersecretion stimulate insulin resistance [14]. The principal mechanism by which the inflammatory signals interfere with insulin action involves post translational modification of insulin receptor substrate molecules particularly via serine phosphorylation that block insulin action. The enzyme c-Jun N-terminal kinase (JNK) is a central mediator, and the endoplasmic reticulum (ER) plays a central role in integrating multiple metabolic signals critical in cellular homeostasis. Therefore, conditions that challenge ER function such as hyperglycaemia in surgical stress would cause glucose overload in the mitochondria, blocks glycolysis and Kreb’s cycle resulting in a further cytokine release and thus creating a vicious cycle [15]. The hyperglycaemia of stress was termed ‘diabetes of injury’ in the 20th century. The deleterious clinical sequelae is quickly manifested in organs with no insulin receptors nor storage capacity such as the kidneys, endothelial of blood vessels and heart, blood cells and neural tissue. However, it responds drastically to insulin treatment as compared to ordinary (atraumatic) patients with non-insulin dependent (type 2) diabetes [16]. The new insight of enhancing recovery after major elective surgery is based on the principle of reducing metabolic stress in surgery by limiting the initiating factors i.e. (1) cytokines produced from tissue injury, and (2) stress hormones from the hypothalamic- pituitary-adrenal axis (HPA) [17,18]. In addition, pre-operative carbohydrate drink and early post-operative feeding and not fasting decreases insulin resistance and puts the patient in an anabolic state. This would diminish the catabolic response to surgery and prevent postoperative hyperglycaemia with its sequelae.
Figure 1: Claude Bernard (French Physiologist) 1813-1878(with permission: www.britannica.com)

Figure 2: Claude Bernard giving a lesson in Physiology (with permission: www.britannica.com)

Figure 3: Ludwig’s wave recording kymograph (1847) (with permission: www.britannica.com)
Sir Michael Foster (1836-1907) (figure 4) was an English physiologist and educator who introduced modern methods of teaching biology and physiology that emphasise laboratory training. Foster earned a medical degree from University College London, in 1859, was a student of the biologist T.H. Huxley, became a teacher (1870-83) and the first professor of physiology (1983-1903) at the University of Cambridge. As initially professor of practical physiology at University College London, he taught the first laboratory course as a regular part of instruction in Medicine which was copied by medical schools in Great Britain and the United States. His research centred on the intrinsic rhythmic activity of the heart and his ‘Textbook of Physiology’ (1877) became a standard reference work. His laboratory produced many of the leading physiologists of the late 19th century and early 20th century in Great Britain and, the United States. In 1876, partly in response to increased opposition in England to experimentation with animals Foster was instrumental in founding the physiological society, the first organization of professional physiologists and in 1878 the Journal of physiology, devoted exclusively to the publication of research results in physiology [19].

Figure 4: Sir Michael Foster (1836-1907) British Physiologist (with permission: www.britannica.com)
The American tradition drew also on the continental schools. S. Weir Mitchell who studied under Claude Bernard, and Henry P. Bowditch, who worked with Carl Ludwig in Germany, joined with Henry Newell Martin a Professor of Biology at Johns Hopkins University in Baltimore and influenced by Foster organized the American Physiological Society in 1867 and the American Journal of Physiology in 1868. Eduard Pfluger, Professor at the Institute of Physiology at Bonn, in 1868, likewise founded the extremely popular ‘Archiv fur de gesammte physiologie’ in Germany. Muller and Liebig provided a stronger relationship between physical and chemical approaches to physiology in Germany. The American tradition in physiological chemistry followed, and in England it developed from a Cambridge laboratory founded in 1898 to complement the physical approach started earlier by Foster.
Caediovascular and Respiratory reflexes: One of the most important cardiac reflexes is the instantaneous reflex control of arterial blood pressure (figure 5). Through adjusting the force and frequency with which the heart ejects blood into the arterial system and thus prevent a raised arterial blood pressure in systole, the baroreceptor reflex is vital for survival.

Figure 5: Schematic diagram of reflex control of cardiac output and peripheral resistance. Baroreceptors in the carotid sinus and aortic arch send information to the brainstem via sensory nerves. Appropriate alterations to parasympathetic and sympathetic activity are made in the medulla oblongata, where preganglionic neurons are located (with permission: www.wlkipaedia)
In 1852, Claude Bernard had discussed that the sympathetic nerves innervate the blood vessels of the skin of the rabbit in addition to its important role in thermoregulation. In the 19th century, Ludwig Traube and Karl Constantine Ewald Hering (figure 6) (1834-1918) discovered that blood pressure fluctuates synchronously with respiratory movements due to variations in vasomotor tone and, that inflating the lungs trigger the acceleration of the heart (Traube-Hering reflex). Sigmund Mayer also observed slow non- respiratory fluctuations of blood pressure. In 1921, Heinrich Ewald Hering (1866-1948), the son of Karl Constantine Ewald Hering found that stretch (baro) receptors are located in the carotid sinus demonstrated by the stimulation of the afferent glossopharyngeal nerve (CN IX) [21]. Through an inhibitory impulse to the cardio-inhibitory and vasomotor centres in the medulla oblongata, inhibition of the sympathetic outflow and stimulation of the parasympathetic outflow, bradycardia and hypotension are induced during increased arterial blood pressure (figure 5). Edgar Douglas Adrian in 1932 demonstrated that the sympathetic nerves that innervate the blood vessels discharge spontaneously at a rate of 4-6 per second which forms the physiological basis of the vasomotor tone. These cardiovascular reflexes were further advanced by Cornielle Heymans who won the Nobel prize in 1938. Later Cowley and Guyton produced sino-aortic denervation in dogs. They demonstrated the baroreceptor reflex involving the baroreceptors in the arch of the aorta innervated by the vagus (X) nerve and the fundamental importance in stabilization of blood pressure [20].

Figure 6: Karl Constantine Ewald Hering (1834-1918) (with permission: www.britannica.com)
Karl Constantine Ewald Hering at the German University in Prague, had supervised a year’s work by Josef Breuer (figure 7) which led to the classic paper on the control of breathing through the vagus nerves [21]. In the Hering-Breuer inflation reflex (figure 8) in 1868 [22], inflation of the lungs produce the usual inhibition of inspiration. Thus it is a reflex triggered to prevent the over-inflation of the lung. Josef Breuer (1842-1925) had shown that inflation of the lungs inhibits and deflation stimulates inspiration (the inflation and deflation Hering- Breuer reflexes), thus establishing the mechanism of the vagal reflex control of the pattern of breathing. Pulmonary stretch receptors present on the wall of bronchi and bronchioles respond to excessive stretching of the lung during large inspirations. Once activated, they send action potentials through large myelinated fibres of the vagus nerve to depress the inspiratory centres in the medulla and withdrawal of outgoing impulses to respiratory muscles and thus allow expiration to occur [23].

Figure 7: Josef Breuer (Austrian physician and physiologist) 1842-1925 (with permission: www.britannica.com)

Figure 8: Schematic diagram of Hering-Breuer reflex (with permission: www.wilkipaedia)
In 1884, Henry Head (1861-1940) (figure 9) interrupted his medical studies in Cambridge, England to do research with Karl Constantine Ewald Hering. Head demonstrated in 1889 that inflation of the lungs produced a situation when the animal actively encouraged inflation (inspiratory activity). This occurred when the vagi nerve had been cooled to between 110 and 50 C. Head took advantage of the method of Gad in 1880 in reversibly blocking the vagus nerves by cold, so that controls could be done before and after blockade [24-27]. More importantly, being a respiratory muscle, he established a method of recording diaphragm contraction from an isolated xiphisternal muscle slip (Heads diaphragm slip preparation). He thus described the ‘paradoxical reflex’ when the vagus nerves were recovering from cold block as inflation of the lungs no longer inhibited inspiration (Hering-Breuer inflation reflex (Figure 10a), but strongly augmented it (Figure 10b). The strength of the inspiratory contractions is not increased but their duration is prolonged, and a tonic inspiratory contraction appeared during the inflation [28]. Vagal section or further cooling abolished the response. Earlier Breuer had confirmed that occasionally, quite contrary to expectation, an animal responded to distension of the lung by air inflation with an inspiration instead of an expiration. Being an innovator Head made and used a “woodcut” cuffed endobronchial tube of rabbit size, which was useful when one lung was either inflated or deflated for a very long period of time while the animal was adequately oxygenated [29]. Fifty years later, it was re-introduced in anaesthesia for humans [24]. In 1946, Larrabee and Knowlton [30] analysed the sensory mechanism of the paradoxical reflex. They showed that it was mediated by rapidly adapting pulmonary stretch receptors (RARs) in the lungs, with properties quite distinct from those of the slowly adapting receptors (SARS) responsible for the Hering-Breuer inflation reflex. The sensory side of the Hering-Breuer reflex is carried by large myelinated fibres with rapid conduction velocities which lose their function between 15 and 90 C, whereas the Head’s paradoxical reflex is carried in small unmyelinated fibres with slow conduction velocities which cease to conduct at considerably lower temperatures between 11 and 50 C. The Head’s paradoxical reflex was intriguing and exciting to me as a physiology student of George Darlow at Bedford College, University of London from 1982-1985. This was because Head’s paradoxical reflex is one of the few examples of positive feedback in the nervous system. George Darlow reproduced these experiments in the physiology laboratory of Bedford College and discussed the possible manifestations in human of this reflex. He reiterated the hypothesis by Cross in 1961 that the Head’s paradoxical reflex although vestigial in the adult was of quite vital importance in the newborn. It manifests in the gasping response (vigorous inspiratory movement) in the newborn baby so as to counteract the surface tension of the fluid in the lungs. Thus, the first breath of a baby is associated with opening up the collapsed lungs so as to get a lot of air in its lungs. The noise of crying is the expiratory activity that follows. This could be explained by the suggestion that the vagi are not fully mature at birth and equivalent to the cooled vagi at a specific temperature of 60 C [28].
The Head’s paradoxical reflex may also be observed in the augmented breaths (gasping) in adults that reverse the tendency of the lungs to collapse during quiet breathing [23] and, the tonic vagal expiratory facilitation is lower in high-altitude infants than low-attitude infants, presumably because of hypoxia [24]. Interestingly, Head proved experimentally that if both lungs are made to collapse suddenly by puncturing the thorax a much stronger inspiratory effort is produced than if both vagi were divided although both operative procedures equally removed the inhibitory stimuli normally passing up the vagi from the lungs. The differences could be explained by assuming that it is the collapse of the lung below the normal volume that produced an actual inspiratory stimulus [25,26]. Head demonstrated that both the paradoxical and the deflation reflex are made possible by the use of the diaphragm slip preparation and vagal cooling. Larrabee and Knowlton in 1946 and later workers analysed the mechanisms and significance of this separate deflation reflex. They showed that the same sensory receptors, the RARs, mediated both reflexes. They were activated by both lung inflations and deflations, and reflexly caused inspiratory activity [29]. In 1895, Hering succeeded Carl Ludwig at the Instutute of Leipzig for the rest of his life studying colour phenomena. Interestingly, Josef Breuer encouraged by Sigmund Freud ended up as a founder of psychoanalysis, whereas Henry Head ended up at the Institute of Neurology, Queen Square, London as the most distinguished neurologist of the 20th century. Experimental physiology had taught him the scientific method and critique which he acknowledged in the preface of his book on aphasia dedicated to Karl Constantine Ewald Hering.

Figure 9: Henry Head FRS (1861-1940) (with permission: www.britannica.com/biography)
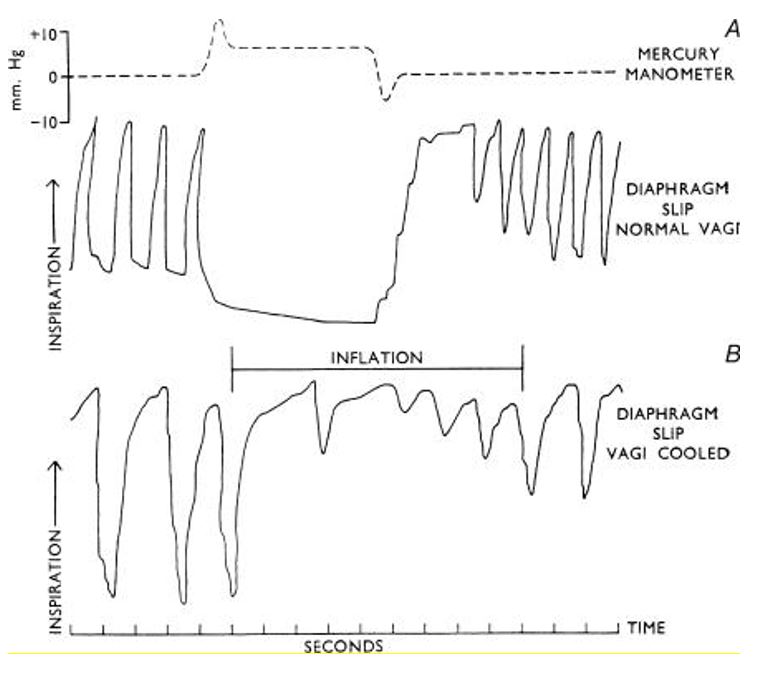
Figures 10a,b: The uppermost trace shows inflation pressure. The lower traces contractions of the diaphragm slip. A, the Breuer- Hering reflex, showing relaxation of the diaphragm. B. Head’s paradoxical reflex, showing contraction of the slip when the vagi were recovering from cold block (with permission: Cross KW. Head’s paradoxical reflex, Brain 84, 529-534)
Ernest Henry Starling (1866-1927) (Figure 11), the English physician and physiologist was one of the foremost scientists of his time [31]. He contributed prolifically to a modern understanding of body functions especially the maintenance of a fluid balance throughout the tissues, the regulatory role of endocrine secretions and the mechanical controls on heart function. While serving as an instructor at Guy’s hospital, London (1889-99) he undertook investigations of lymph secretion that resulted in the clarification of the nature of fluid exchanges between vessels and tissues. Using physico-chemical principles he demonstrated the balance between colloidal (protein) osmotic pressure forcing an absorption of fluid from the tissues through the semi-permeable capillaries and hydrostatic pressure forcing these solutions into tissues- the Starling hypothesis (1896) [32]. As Professor of Physiology at University College London (1899-1923) he collaborated with the British physiologist, William Bayliss in 1899 to demonstrate the nervous control of the peristaltic wave responsible for the movement of food through the intestine [33,34]. He coined the term ‘hormone’ following the isolation in 1902 of secretin released into the blood from the epithelial cells of the duodenum mainly in response to the acidic gastric chyme which in turn stimulates pancreatic secretion of a high volume of alkaline (bicarbonate) rich fluid to neutralize this acid [35]. Starling developed an isolated heart-lung preparation for a World War 1 poison gas defense research. This enabled him to formulate the “Starling’s law of the heart’ in 1918 which stated that the force of muscular contraction of the heart is directly proportional to the extent to which it is stretched. This has implications on cardiovascular disease and therapeutics [36]. His study on kidney function in 1924 demonstrated that the water, chlorides, bicarbonates, and glucose, lost in the excretory filtrate, are reabsorbed at the lower end of the kidney tubules of the nephron [37].
Figure 11: Ernest Henry Starling 1866-1927 (British Physiologist) (with permission: www.britannica.com)
Physiology in the 20th century was a mature science. During a century of growth, physiology became the parent of a number of related disciplines, of which biochemistry, biophysics, general physiology, and molecular biology are the most vigorous examples. It retained an important position among the functional sciences that are closely related to the field of medicine. Unsolved problems of physiology will require technical and expensive research by teams of specialized investigators. For example, at the turn of the 20th century, in1921, Dr Frederick Banting (1891-1941), a Canadian surgeon and Charles Best, a medical student, successfully isolated the hormone insulin from the beta islet cells of Langerhan in the pancreas under the directorship of John Macleod (1876-1935), a Scottish Physiologist at the University of Toronto. John Macleod received his medical training at the University of Aberdeen in 1898 and biochemical training at the Institute for physiology at the University of Liepzig and became an expert in carbohydrate metabolism. In 1922, a 14-year old boy became the first person to receive an insulin injection as treatment for diabetes mellitus, and, in 1923, Banting and Macleod were awarded the Noble prize [38].
Neurophysiology
With regard to the central nervous system, Sir Charles Scott Sherrington (1857-1952) (Figure 12) an English physician and physiologist’s 50 year of experimentation laid the foundations for an understanding of the integrated nervous function in higher animals. Sherrington found that reflexes must be regarded as integrated activities of the total organism and not as the result of the activities of isolated ‘reflex arcs’. His first major piece of evidence supporting ‘total integration’ was the demonstration (1895-98) of the ‘reciprocal innervation’ of muscles also known as Sherrington’s law: when one set of muscles is stimulated, muscles opposing the action of the first are simultaneously inhibited [39]. Along with Edgar Adrian he won the Nobel prize in 1932. Sherrington was born in London, educated at Cambridge, a student of Michael Foster and qualified in medicine at St Thomas’s hospital medical school in 1885. He worked with Rudolf Virchow and Robert Koch at the University of Berlin and was successively a professor at the Universities of London (1891-95), Liverpool (1895-1913) and Oxford (1913-35). His investigations of nearly every aspect of mammalian nervous system including the study on the maintenance of posture against gravity as a reflex activity by the muscles’ proprioceptors and their nerve trunks despite the removal of the cerebrum (decerebrate rigidity) influenced the development of brain surgery, and the treatment of paralysis and atrophy [40]. He coined the term ‘synapse’ to denote the point at which the nervous impulse is transmitted from one nerve cell to another [41].

Figure 12: Sir Charles Scott Sherrington 1857-1952 (British Physiologist) (with permission: www.britannica.com)
The plasticity of synaptic connections is a known exceptional ability of the brain to respond dynamically to stimuli [42-44]. Due to its relation to learning and memory formation, as well as recovery from brain injury and the aberrant expressions in neuropsychiatric disorders such as Alzheimer’s disease, multiple sclerosis [45-49], ongoing research into synaptic plasticity is essential in providing key insights into the difference between normal and pathological brain function. It may also provide the understanding of the biological basis of gut motility disorders ranging from pseudo-obstruction in the newborn to Hirschsprung’s disease, the metastatic process of cancer and aspects of human psychology [45,50] .The neural cell adhesion molecule (NCAM) is another essential factor governing synaptic plasticity through replay of neurodevelopmental events [45]. It is a single pass trans-membrane glycoprotein belonging to the immunoglobulin super family which is transiently expressed in many tissues within the central and peripheral nervous systems and skeletal muscles during early embryogenesis, where it plays an essential role in neural development before demonstrating a more limited expression pattern upon maturity [51]. Monoclonal antibodies against NCAM is currently used diagnostically and therapeutically [45,52]. Neuroplasticity also occurs in the peripheral nervous system and skeletal muscles as demonstrated in the modification of ‘fast’ and ‘slow’ type skeletal muscles during exercise training [53] or electrical stimulation as seen in the stimulated graciloplasty as a neo-anal sphincter [54] and, the continuous low frequency simultaneous pacing of both hemi-diaphragms as a satisfactory method of providing full-time ventilator support [55].
The neuroscientist, Gerta Vrbova (1926-2020) (figure 13) was born in Slovakia and graduated from medical studies at the Charles University in Prague in 1950. She was a holocaust survivor and with her mentor Ernest Gutmann (1919-1977) at the Institute of Physiology of the Czechoslovak Academy of Sciences worked on nerve-muscle interaction early in Prague [56]. She continued her work initially at the Royal Free Hospital, London on the physiology of neuromuscular depolarizing drugs which led to innovations in anaesthesia. She demonstrated many molecular and metabolic events that occur by changing the pattern of activation of muscle fibres through neuromuscular low frequency electrical stimulation [55]. She became a professor of developmental neuroscience at the University College London in 1976. At the Centre of Neuroscience, University College London (1985-86), I was privileged to have her supervise my Master of Neurological science (MSc) thesis on the development of motoneurones in the lumbo-sacral segments of the rat’s spinal cord. Her work on the differentiation and extent of plasticity of peculiar characteristics of the different types of fibres present in mammalian muscles led her research groups in the Universities of Birmingham and London develop electrical muscle stimulators that are widely used today in rehabilitation and sport [55,57].

Figure 13: Gerta Vrbova (1926-2020) Neuroscientist (with permission: www.britannica.com)
With regard to our knowledge of the somatosensory system and in particular, pain mechanisms, a tribute must be given to Patrick David Wall (1925-2001) (Figure 14). He was a British neuroscientist born in Nottingham, described as the world’s leading expert on pain and best known for the ‘gate control theory of pain’. The gate control theory of pain asserts that non-painful input closes the nerve “gates” to painful input, which prevents pain sensation from traveling to the central nervous system. First proposed in 1965 by Ronald Melzack and Patrick Wall, the theory offers a physiological explanation for the previously observed effect of psychology on pain perception [58], and the traditional Chinese practice of acupuncture [59]. It provided a neural basis which reconciled the specificity and peripheral pattern theories that ultimately revolutionized pain research [60]. The peripheral nervous system has centres in the spinal cord where pain stimuli can be regulated. Some areas in the dorsal horn of the spinal cord (substantia gelatinosa) are involved in receiving pain stimuli from Aδ and C fibres, called laminae. They also receive input from the non-nociceptive fibres which indirectly inhibit the effects of the pain fibres through local interneurones. Thus, ‘closing a gate’ to the transmission of their stimuli. In other parts of the laminae, pain fibres also inhibit the effects of nonnociceptive fibres, ‘opening the gate’. Certain gamma amino butyric acid (GABAα) receptor subtypes but not glycine receptors can presynaptically regulate nociception and pain transmission . Thus, depending on the relative rates of firing of C and Aβ fibres, the firing of the non-nociceptive fibre may inhibit the firing of the projection neuron and the transmission of pain stimuli [61]. Patrick Wall studied Medicine in Christ Church, Oxford University where he became interested in pain and published his first two papers, in the prominent science journals Brain and Nature at the age of 21.
He graduated in Medicine in 1948 and took up a position as an instructor at the Yale School of Medicine investigating the use of lobotomies as a method of controlling depression. In 1965, he was Professor of Anatomy at University College London and in 1972 also held a chair at the Hebrew University of Jerusalem. His laboratories attracted a large number of students and researchers [62]. His lectures were well received by both students including myself and his fellow lecturers. In 1982, he published with Melzack ‘The challenge of Pain” followed by a second collaboration a year later with “The textbook of pain”, which is currently in its fifth edition [63]. I was fortunate to accompany him during his regular consultations of World War 2 veterans with chronic pain at the nearby Middlesex hospital. Apart from being listed for the Nobel prize, he was awarded the Sherrington Medal of the Royal Society of Medicine in 1988, elected as fellow of the Royal College of Anesthesiologists in 1992 and, received in 1999 the Royal medal from the Royal Society for his contributions to the advancement of natural knowledge. While suffering from prostate cancer he published the book ‘Pain: The Science of Suffering” [64], and donated his body for scientific teaching and research.
Figure 14: Patrick David Wall (1925-2001) British Neuroscientist (with permission: www.britannica.com)
|
Table 1: Aspects of experimental physiology (17th century to 20th century) |
||
|
Period |
Scientist |
Discovery |
|
17th century
!8th Century
19th Century
20th Century
|
William Harvey (1628) Marcello Malpighi (1667) Albrecht von Haller (1747) Antoine Lavoisier (1789) Claude Bernard (1813-1878) Johannes Muller (1834) Justus von Liebeg (1840) Carl Ludwig (1847) Karl Ewald.Hering( 1869) Josef Breuer (1868) Michael Foster (1877) Henry Head (1884) Ivan Pavlov (1890) Ernest Starling (1896)
William Bayliss (1902) Banting and Macleod (1921) William B Cannon(1932) Charles S, Sherrington (1932) Edgar Douglas Adrian(1932) Heinrich Ewald Hering (1948) Cowley & Guyton (1973) Patrick David Wall (1965) Gerta Vrbova (1979) |
Circulation Capillaries first manual on Physiology combustion and respiration Homeostasis Experimental physiology Physiological chemistry Cardiovascular physiology Traube-Hering reflex Hering-Breuer reflex Practical physiology Head’s paradoxical reflex Conditioned reflexes Starling’s law of the heart
Autonomic peptide (secretin) Diabetes mellitus (Insulin) ‘fight or flight’ response Integrated spinal reflexes Vasomotor tone Carotid sinus baroreflex arc Sinoaortic baroreflex arc Gate-control theory of pain Nerve-muscle interaction |
Conclusions
Experimental physiology demonstrates the normal function of the body systems by using the scientific method. Many diseases are natural experiments and thus the important corollary to the physician’s ability to recognize and evaluate the abnormal, and take intelligent action to prevent, compensate for, and cure departures from normality. There is equal importance of the scientist and the physician. The interaction and collaboration between the scientist who aims to understand the functioning of the human body and the physician who aims to treat the malfunction is mandatory in modern medicine. This is corroborated by the fact that medicine is an art based on science. The optimum would be being both a scientist and physician as seen with these legends. Their legacies will live forever.
References
1. Bayliss LE. 1959. Principles of General Physiology.
2. Bolli R. 2019. William Harvey and the discovery of the circulation of the blood. Circulation research. 124: 1300-1302. Ref.: https://pubmed.ncbi.nlm.nih.gov/31021729/ DOI: https://doi.org/10.1161/circresaha.119.314977
3. Pearce JMS. 2007. Malpighi and the discovery of capillaries. Eur Neurol. 58: 253-255. Ref.: https://pubmed.ncbi.nlm.nih.gov/24217847/ DOI: https://doi.org/10.7417/ct.2013.1625
4. Conti AA. 2013. Albrecht von Haller: an encyclopaedic cosmopolite in the history of Swiss medicine. Clin Ter. 164: 445-448. Ref.: https://pubmed.ncbi.nlm.nih.gov/24217847/ DOI: https://doi.org/10.7417/ct.2013.1625
5. Holmes FL. 1985. Lavoisier and the chemistry of life. Madison, Wisconsin: Universty of Wisconsin Press.
6. Bernard C, Magendie F. 1856. Lecon d’ouverture du cours de Medecine du College de France. Bailliere, Paris.
7. Bell C, Shaw A. 1868. Reprint of the “Idea of a New Anatomy of the Brain” with Letters.&c. J Anat Physiol. 3: 147-182. Ref.: https://pubmed.ncbi.nlm.nih.gov/17230788/
8. Noble D. 2008. Claude Bernard, the first systems biologist and the future of physiology. Exp Physiol 93: 16-26. Ref.: https://pubmed.ncbi.nlm.nih.gov/17951329/ DOI: https://doi.org/10.1113/expphysiol.2007.038695
9. Todes DP. 1997. Pavlov’s Physiological factory. The History of Science society. 88: 205-246. Ref.: https://pubmed.ncbi.nlm.nih.gov/9325628/ DOI: https://doi.org/10.1086/383690
10. Billman GE. 2020. Homeostasis: The underappreciated and far too often ignored central organizing principle of physiology. Front Physiol. 11: 200. Ref.: https://pubmed.ncbi.nlm.nih.gov/32210840/ DOI: https://doi.org/10.3389/fphys.2020.00200
11. Bernard C. 1877. Hyperglycaemia in haemorrhage. Paris Baillier. 210.
12. Ljungvist O, Alibegovic A. 1994. Hyperglycaemia and survival after haemorrhage. Eur J Surg. 160: 465-469. Ref.: https://pubmed.ncbi.nlm.nih.gov/7849164/
13. Cannon W. 1932. Wisdom of the body. United States: WW Norton & Company.
14. Thorell A, Nygren J, Ljungqvist O. 1999. Insulin resistance, a marker of surgical stress. Curr Opin Clin Nutr Metab Care. 2: 69-78. Ref.: https://pubmed.ncbi.nlm.nih.gov/10453333/ DOI: https://doi.org/10.1097/00075197-199901000-00012
15. Vallerie SN, Furuhashi M, Fucho R. 2008. A predominant role for parenchymal c-Jun amino terminal kinase (JNK) in the regulation of systemic insulin sensitivity. PLoS ONE. 3: 3151. Ref.: https://pubmed.ncbi.nlm.nih.gov/18773087/ DOI: https://doi.org/10.1371/journal.pone.0003151
16. Lassen K, Soop M, Nygren J. 2009. Consensus review of optimal perioperative care in colorectal surgery; Enhanced Recovery after surgery (ERAS) recommendation. Arch Surg. 144: 961-969. Ref.: https://pubmed.ncbi.nlm.nih.gov/19841366/ DOI: https://doi.org/10.1001/archsurg.2009.170
17. Weledji EP. 2014. Cytokines and postoperative hyperglycaemia: from Claude Bernard to enhanced recovery after surgery. Int J Surgical Research. 3: 1-6.
18. Weledji EP, Njong S, Chichom AM. 2017. The effects of preoperative carbohydrate loading on the metabolic response to surgery in a low resource setting. Int J of Surg. 8: 18-23.
19. Hawgood BJ. 2008. Sir Michael Foster MD, FRS (1836-1907): The rise of the British school of Physiology. J of Med Biography England. 15: 821-826. Ref.: https://pubmed.ncbi.nlm.nih.gov/18952994/ DOI: https://doi.org/10.1258/jmb.2008.008009
20. Bruno E. Porvas BM, Padilla LMA. 2011. A brief history of the baroreceptor reflex: from Claude Bernard to Arthur C Guyton: illustrated with some classical experiments. Arch Cardiol Mex. 81: 330-336. Ref.: https://pubmed.ncbi.nlm.nih.gov/22188890/
21. Breuer J. 1886. Self- steering of respiration through the nervus vagus. Sber Akad Wiss Wien. 58: 909-937.
22. West J. 2015. Respiratory physiology: the essentials. Hagerstown, MD: Lippincott Williams & Wilkins. 127-128.
23. Widdicombe J. 2004. Henry Head and his paradoxical reflex. J Physiol. 559: 1-2. Ref.: https://pubmed.ncbi.nlm.nih.gov/15121807/ DOI: https://doi.org/10.1113/jphysiol.2004.065367
24. Mortola JP, Trippenbach T, Rezonico R. 1995. Hering-Breuer reflexes in high-altitude infants. Clin Sci (Lond). 88: 345-350. Ref.: https://pubmed.ncbi.nlm.nih.gov/7736705/ DOI: https://doi.org/10.1042/cs0880345
25. Zechman Jr, Salzano J, Hall F. 1958. Effect of cooling the cervical vagi on the work of breathing. J Applied Physiol. 12: 301. Ref.: https://pubmed.ncbi.nlm.nih.gov/13525278/ DOI: https://doi.org/10.1152/jappl.1958.12.2.301
26. Head H. 1889. On the regulation of respiration: Part 1 Experimental. J Physiol. 10: 1-70.
27. Head H. 1889. On the regulation of respiration Part II Theoretical. J Physiol. 10: 279-290. Ref.: https://pubmed.ncbi.nlm.nih.gov/16991889/ DOI: https://doi.org/10.1113/jphysiol.1889.sp000304
28. Cross KW. 1961. Head’s paradoxical reflex. Brain. 84: 529-534. Ref.: https://pubmed.ncbi.nlm.nih.gov/13882382/ DOI: https://doi.org/10.1093/brain/84.4.529
29. Larrabee MG, Knowlton GC. 1946. Excitation and inhibition of phrenic motoneurones by inflation of the lungs. Am J Physiol. 147: 90-99. Ref.: https://pubmed.ncbi.nlm.nih.gov/21000727/ DOI: https://doi.org/10.1152/ajplegacy.1946.147.1.90
30. Davies A, Roumy M. 1982. The effect of transient stimulation of lung irritant receptors on the pattern of breathing in rabbits. J Physiol. 324: 389-401. Ref.: https://pubmed.ncbi.nlm.nih.gov/7097605/ DOI: https://doi.org/10.1113/jphysiol.1982.sp014119
31. Henriksen JH. 2005. Ernest Henry Starling (1866-1927): the scientist and the man. J Med Biogr. 13: 22-30. Ref.: https://pubmed.ncbi.nlm.nih.gov/15682229/ DOI: https://doi.org/10.1177/096777200501300107
32. Rodney LJ, Charles MC. 2010. Microvascular fluid exchange and the revised Starling principle. Cardiovasc Res. 87: 198-210. Ref.: https://pubmed.ncbi.nlm.nih.gov/20200043/ DOI: https://doi.org/10.1093/cvr/cvq062
33. Bayliss WM, Starling EH. 1899. The movements and innervations of the small intestine. J Physiol. 24: 99. Ref.: https://pubmed.ncbi.nlm.nih.gov/16992487/ DOI: https://doi.org/10.1113/jphysiol.1899.sp000752
34. Weledji EP. 2020. Perspectives on paralytic ileus. Acute Med Surg. 7: 573. Ref.: https://pubmed.ncbi.nlm.nih.gov/33024568/ DOI: https://doi.org/10.1002/ams2.573
35. Modlin I. 2001. Ernest Starling and the discovery of secretin. J of Clin Gastroenterol. 32: 187-192. Ref.: https://pubmed.ncbi.nlm.nih.gov/11246341/ DOI: https://doi.org/10.1097/00004836-200103000-00001
36. Han JC, Phm T, Taberner AJ. 2019. Solving a century-old conundrum underlying cardiac force-length relations. Am J Physiol Heart Circ Physiol. 316: 781-793. Ref.: https://pubmed.ncbi.nlm.nih.gov/30707611/ DOI: https://doi.org/10.1152/ajpheart.00763.2018
37. Fine LG. 2014. Ernest Henry Starling (1866-1927) on the glomerular and tubular functions of the kidney. Nephron Physiol. 126: 19-28. Ref.: https://pubmed.ncbi.nlm.nih.gov/24970544/ DOI: https://doi.org/10.1159/000363302
38. Home P. 2021. The evolution of insulin therapy. Diabetes Research and clinical practice. 175: 108816. Ref.: https://pubmed.ncbi.nlm.nih.gov/33862058/ DOI: https://doi.org/10.1016/j.diabres.2021.108816
39. Sherrington CS. 1893. Further experimental note on the correlation of action of antagonistic muscles. Br Med J. 1: 1218.
40. Louis ED. 2020. The Sherrington- Cushing connection: A bench to bedside collaboration at the dawn of the twentieth century. J Hist Neurosc. 29: 203-220. Ref.: https://pubmed.ncbi.nlm.nih.gov/31503517/ DOI: https://doi.org/10.1080/0964704x.2019.1656377
41. Creed RS, Denny BD, Eccles JC. 1932. Reflex activity of the spinal cord. Clarendon Press.
42. Citri A, Malenka RC. 2008. Synaptic plasticity: multiple forms, functions, and mechanisms. Neuropharmacology. 33: 18-41. Ref.: https://pubmed.ncbi.nlm.nih.gov/17728696/ DOI: https://doi.org/10.1038/sj.npp.1301559
43. Ho V, Lee J, Martin K. 2011. The cell biology of synaptic plasticity. Science. 334: 623-628. Ref.: https://pubmed.ncbi.nlm.nih.gov/22053042/ DOI: https://doi.org/10.1126/science.1209236
44. Frohlich F. 2016. Synaptic plasticity. Network Neuroscience. 47-58.
45. Weledji EP, Assob JC. 2014. The ubiquitous neural cell adhesion molecule (NCAM). Ann Med Surg (Lond). 3: 77-81. Ref.: https://pubmed.ncbi.nlm.nih.gov/25568792/ DOI: https://doi.org/10.1016/j.amsu.2014.06.014
46. Leschchyns’ka I, Sytnyk V. 2016. Synaptic cell adhesion molecules in Ahzheimer’s disease Neural Plast. 6427537. Ref.: https://pubmed.ncbi.nlm.nih.gov/27242933/ DOI: https://doi.org/10.1155/2016/6427537
47. Brennaman CH, Maness PF. 2010. NCAM in neuropsychiatric and neurodegenerative disorders. Adv Exp Med Biol. 2663: 299-317. Ref.: https://pubmed.ncbi.nlm.nih.gov/20017030/ DOI: https://doi.org/10.1007/978-1-4419-1170-4_19
48. Granapavan S, Ho P, Heywood W. 2013. Progression in multiple sclerosis is associated with low endogeneous NCAM. J Neurochem. 125: 766-773. Ref.: https://pubmed.ncbi.nlm.nih.gov/23495921/ DOI: https://doi.org/10.1111/jnc.12236
49. Weledji EP, Regan CM. 2014. The Neuroanatomical localization of a specific memory. Int J Brain and Cognitive Sciences. 3: 44-49.
50. Weledji EP, Ngo NB. 2013. Pseudo-obstruction in the neonate- a difficult diagnosis in a poor-resourced area. J Ped Surg case Rep. 1: 258-259.
51. Weledji EP. 2018. The neural cell adhesion molecule (NCAM): from memory formation to cancer. Arch Clin Pathol. 1: 1.
52. Kaufmann O, Georgi T, Dietel M. 1997. Utility of 123C3 monoclonal antibody against CD56 (NCAM) for the diagnosis of small cell carcinomas on paraffin sections. Hum Pathol. 28: 1373-1378. Ref.: https://pubmed.ncbi.nlm.nih.gov/9416693/ DOI: https://doi.org/10.1016/s0046-8177(97)90226-4
53. Weledji EP, Assob JC, Siysi VV. 2013. How to improve performance in sport- a review. J Phys Pharm Adv. 5: 131-138.
54. Mavrantonis C, Billotti VL Wexner SD. 1999. Stimulated graciloplasty for treatment of intractable fecal incontinence: critical influence of the method of stimulation”. Dis Colon Rectum. 42: 497-504. Ref.: https://pubmed.ncbi.nlm.nih.gov/10215051/ DOI: https://doi.org/10.1007/bf02234176
55. Pette D. 2021. The significance of Gerta Vrbova’s low frequency stimulation experiment” Eur J Transl Myol. 31: 9585. Ref.: https://pubmed.ncbi.nlm.nih.gov/33709646/ DOI: https://doi.org/10.4081/ejtm.2021.9585
56. Vrbova G, Koffer GA, Pette D. 2008. Ernest Gutmann (1910-1977). Neurol Res. 30: 117-118. Ref.: https://pubmed.ncbi.nlm.nih.gov/18397600/ DOI: https://doi.org/10.1179/174313208x281118
57. Vrbova G, Gordon T, Jones R. 1994. Nerve-muscle interaction; eds Gerta Vrbova, Tessa Gordon, Rosie Jones. edn 2 Springer Netherlands.
58. Melzack R, Wall PD. 1965. Pain mechanisms: a new theory. Science.150: 971-979. Ref.: https://pubmed.ncbi.nlm.nih.gov/5320816/ DOI: https://doi.org/10.1126/science.150.3699.971
59. Berman BM, Langevin HM, Witt CM. 2010. Acupuncture for chronic low back pain. N Engl J Med. 363: 454-461. Ref.: https://pubmed.ncbi.nlm.nih.gov/20818865/ DOI: https://doi.org/10.1056/nejmct0806114
60. Moayedi M, Davis KD. Theories of pain: from specificity to gate control. J of Neurophysiology. 109: 5-12. Ref.: https://pubmed.ncbi.nlm.nih.gov/23034364/ DOI: https://doi.org/10.1152/jn.00457.2012
61. Wall PD. 1978. The gate control theory of pain mechanisms: A re-examination and re-statement. Brain. 101: 1-18. Ref.: https://pubmed.ncbi.nlm.nih.gov/205314/ DOI: https://doi.org/10.1093/brain/101.1.1
62. Fitzgerald M. 1978. The sensitization of cutaneous nociceptors (Phd thesis), University College London.
63. Rathmell JP, Hill B. 2006. Wall and Melzack’s Textbook of Pain, 5th edition; eds Ellison, Norig. Aneasthesia & Analgesia. 102: 1914.
64. Obituaries. 2001. James Colquhoun Petrie, Patrick David Wall, Sir William Ferguson Anderson, Denys Elwyn Howells, Ronald Herbert Jones, Paul Alexandra, Koyotsu Padi, William Patrick Reynish. BMJ. 323: 636.


















